Download
1 / 21
210 likes | 393 Views
Depression CDSS. Charles Kitzman , Barbary Baer, Sudha Poosa. The Project. To maximize BH efficiencies while maintaining quality care Workflow optimization FQHC integrated BH m odel Strategic partnership Continuity of care/chart sharing Advanced primary care practice.

E N D
Depression CDSS Charles Kitzman, Barbary Baer, SudhaPoosa
The Project • To maximize BH efficiencies while maintaining quality care • Workflow optimization • FQHC integrated BH model • Strategic partnership • Continuity of care/chart sharing • Advanced primary care practice
Environment • FQHC northern CA county • Woefully inadequate BH services • PH contractual outpatient • Demand > Access • Obligation to have streamlined services • Filter inadequate referrals • Time for appropriate patients
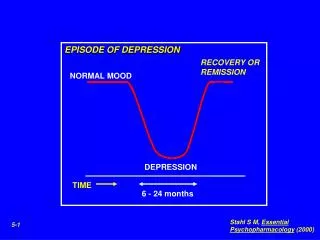
Backdrop Higher rates for Suicide >50% 65 or older
Bottling the ends • Our approach sought to narrow scope • Why? It’s a diverse field with lots of variability. Makes it difficult to study • Many tools, many interpretations • Depression is our focus • PQH-9 and lab results respectively
Rationale for screening • Only half of depressed patients are diagnosed by their primary care physician • Patients with serious mental illness are 23% more likely to have a non-psychiatric hospitalization compared to the rest of the population. At $6000/admission, this adds $16 million to California’s Medi-Cal program • Depression is associated with greater health service use, greater morbidity & mortality, increased medical costs, not to mention unnecessary suffering
PHQ-9 • Advantages • Self-administered • Freely available • Short (9 items) • Has been validated in Spanish • Sensitivity: from 94.4% (cutoff point >= 9) to 88.9% (cutoff point >= 13) • Specificity: from 73.3% (cutoff point >= 9) to 86.7% (cutoff point >= 13) • Original study: • Sensitivity for major depression: 88% for scores > 10 • Specificity for major depression: 88% • Scores of 5, 10, 15, 20 represented mild, moderate, moderately severe, severe depression respectively
System : Input • Demographics • Chief complaint • HPI (History of present illness) • Other illnesses • Medications • Life events
System : Architecture and Interface • Enterprise wide client-server based architecture • Architecture will comprise database and the rules engine • Compliant with standards – HIPAA, LOINC, HL7, etc. • Use of drop menus and logic checks • Use of clinic reminders and alerts • Capability of creating individual care plans with self-management information and disease severity rating • Linked with, but not a substitute for electronic medical records. Will be integrated at the point of care • PHQ-9 entry can be made by the patient, nurse or the clinician
System : Output & Workflow • Context-specific decision support in real time • Test score & risk stratification • Treatment regimen • Whom to refer the patient to (level of BH clinician) • When should the patient be tested / re-evaluated • When to administer medications to the patient • Treatment options • No treatment • Watchful waiting • Psychotherapy / counseling • Anti-depressant medication • Combination therapies
Evaluation • Audit of inappropriate referrals with an expectation of declining numbers • Increased access or an increase in encounters per clinic hour for BH staff • Increase in consistent use of screening tools by PC staff • Log trigger results to check provider compliance with tool suggestions • Better outcomes
Conclusions • Difficult to separate operations from clinical decision piece • BH is very complex field to understand • Actually will beta-test in the clinic with a few providers