Download
1 / 29
380 likes | 767 Views
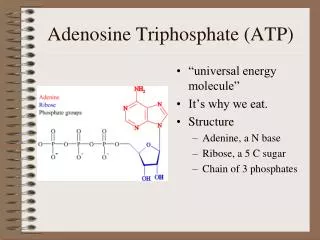
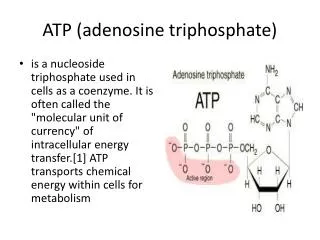
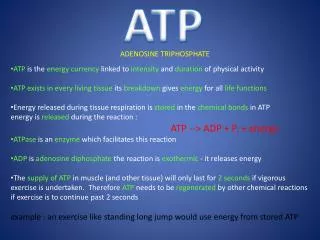
Information Storage (Purine base in DNA). Information Retrieval (Purine base in RNA). Intracellular Signaling (cAMP). Energy Metabolism (ATP/ADP). Adenosine. Communications (Adenosine importantly directs cell-to-cell signaling with significant consequences for organ function.).

E N D
Information Storage (Purine base in DNA) Information Retrieval (Purine base in RNA) Intracellular Signaling (cAMP) Energy Metabolism (ATP/ADP) Adenosine Communications (Adenosine importantly directs cell-to-cell signaling with significant consequences for organ function.)
Adenosine Receptors: SignalTransduction Mechanisms (Low affinity) A2B A3 A1 A2A (Very high affinity) (High affinity) Gs Gq/11 Gi/o alphas alphai beta/gamma alphaq/11 AC K+ Channels (KATP) PLC Subtypes have distinct, but overlapping, cellular distribution and are widely expressed in most cells/tissues/organs of the body. Ca2+ Channels
Adenosine Production: During A Crisis Event CELL ATP ATP Intracellular ATP Pathway ADP ADP AMP AMP Extracellular ATP Pathway ADO ADO
Adenosine Production: Constitutive CELL SAM Methylation Pathway SAH ADO ADO
Adenosine Production: Regulated cAMP Transporter CELL AC Ecto-PDE ATP cAMP AMP cAMP-Adenosine Pathway Ecto-5’NT ADO Paracrine Autocrine
Heart:Protection from reperfusion injury Mervyn B. Forman, MD, PhD, FACC Atlanta Cardiovascular Associates 1,000,000 Americans suffer a heart attack (AMI) annually 200,000 (20%) die during or soon after AMI Survivors: up to 15-fold greater risk of death Survivors: 22% of males and 46% of females are disable by heart failure TOO MUCH HEART DAMAGE IN AFTERMATH OF AMI!!
Angioplasty (with or without stenting) Thrombolytic Therapy Myocardial Reperfusion Injury
Myocardial Reperfusion Injury • Definition: Conversion of reversibly injured endothelial and myocardial cells to irreversibly injured cells during the peri-reperfusion period. Not synonymous with entity of acceleration of necrosis of cells that are already irreversibly injured.
Myocardial Reperfusion Injury • Experimental Evidence of Reperfusion Injury • MRI evidence of time-related infarct extension after reperfusion • Enhanced myocardial salvage with therapeutic agents administered after reperfusion • Differential histology between reperfused and non-reperfused myocardium
A2A/2B Angiogenesis Vasculogenesis ADENOSINE Mechanisms of Myocardial Reperfusion Injury and Effects of Adenosine Reperfusion TxA2, PAF, Ang II, NE, ET-1 Platelets Leukocytes Oxygen Calcium A1/3 A1/3 A2A A2A A2A Oxygen Free Radicals Cellular Calcium Overload MPO Proteases Platelet Aggregation Vasoconstriction Vascular Plugging No Reflow Cell Death
50 Control (n=13) 40 35 ± 4 % 30 AN/AR Adenosine (n=9) (%) 20 17 ± 4 % p<0.01 10 0 Effect of IV Adenosine at Reperfusion on Infarct Size in a Dog Model of AMI Implanted LAD snare in 22 dogs; 5-7 days later, 90-min LAD occlusion in closed-chest dogs; 0.15 mg/kg/min adenosine IV for 150 min starting at reperfusion; AN/AR at 72 hrs post-AMI (Mallory’s trichrome stain/Monastral blue)
Transverse Myocardial Slice in Adenosine and Control Animal Adenosine-Treated Control
Control Adenosine 25 **p<.01 21 ** 20 20 ** 17.3 15 ** Shortening (%) Ischemic Zone Radial 11 10 5.5 5 0 -2.6 -5 Base OCC Rep 3H Rep 72H Regional Ventricular Function in Ischemic Zone Contrast ventriculography and calculation of radial shortening
CONTROL ZONE CENTRAL ZONE **P<0.01 *P<0.05 ENDOCARDIAL FLOW 1.0 2.0 ADENOSINE ADENOSINE Base OCC REP 1 HR 2 HR 24 HR Base OCC REP 1 HR 2 HR 24 HR CONTROL ADENOSINE Endocardial Blood Flow (ml/min/g) in Treated and Control Animals Radioactive microspheres
Bedside • Prospective clinical trials • ATTACC STUDY (Phase 2) • AMISTAD TRIAL (Phase 2) • AMISTAD II TRIAL (Phase 3) Lab Bench
AMISTAD II 13 Countries 390 Study Sites 2118 Patients with Anterior STEMI & Reperfusion Therapy within 6 Hrs of Symptoms Placebo Adenosine 50 μg/Kg/min X 3h Adenosine 70 μg/Kg/min X 3h Fibrinolysis or PTCA Infarct size (5 d) (243 patients) Follow-up for 6 months
Median LV Infarct Size (%) p=0.028 40% p=0.122 30% 26% 23% 20% 11% 10% 0% 50 μg 70 μg Placebo AMISTAD II Infarct Size 57% reduction in median infarct size with 70 μg/kg/min group relative to placebo
Primary Clinical End Points AMISTAD II: INTENT-TO-TREAT JACC 2005, 45: 1775-80.
“…because animal studies demonstrate that adenosine’s beneficial effects are lost if myocardial ischemia occurs for more than 3 h , adenosine would prevent reperfusion injury only in patients receiving adenosine within the first 3 h after coronary occlusion. Therefore, a subset analysis of the adenosine groups who were reperfused within 3 h may yield an even greater reduction in clinical end points.” JACC 47, 1235, March , 2006 (letter to editor of JACC by Forman and Jackson)
European Heart Journal 27: 2400-2405, Oct., 2006 Aims The purpose of this analysis was to determine whether the efficacy of adenosine vs. placebo was dependent on the timing of reperfusion therapy in the second Acute Myocardial Infarction Study of Adenosine (AMISTAD-II). Methods and Results Patients presenting with ST-segment elevation anterior AMI were randomized toreceive placebo vs. adenosine (50 or 70 mg/kg/min) for 3 h starting within 15 min of reperfusiontherapy. In the present post hoc hypothesis generating study, the results were stratified according to the timing of reperfusion, i.e. or , the median 3.17 h, and by reperfusion modality. In patients receiving reperfusion <3.17 h, adenosine compared with placebo significantly reduced 1-month mortality (5.2 vs. 9.2%, respectively, P=0.014), 6-month mortality (7.3 vs. 11.2%, P =0.033), and the occurrence of the primary 6-month composite clinical endpoint of death, in-hospital CHF, or rehospitalization for CHF at 6 months (12.0 vs. 17.2%, P =0.022).Patients reperfused beyond 3 h did not benefit from adenosine. ConclusionIn this post hoc analysis, 3 h adenosine infusion administered as an adjunct to reperfusion therapy within the first 3.17 h onset of evolving anterior ST-segment elevation AMI enhanced early and late survival, and reduced the composite clinical endpoint of death or CHF at 6 months.
DEATH AT 6 MONTHS IF THERAPY WITHIN 3 HOURS Adenosine: 7.3% (n=716) Placebo: 11.2% (n=350) P=0.033 Adenosine: 800,000/y x 0.073 = 58,400/y Placebo: 800,000/y x 0.112 = 89,600/y Lives Saved: 89,600/y – 58,400/y = 31,200/y
Key Points • Adenosine reduces infarct size • Adenosine reduces risk of death AMI patients who undergo reperfusion therapy:
What is the “No-Reflow” Phenomenon? The “no-reflow” phenomenon is defined as impaired tissue perfusion despite successful treatment of the target macrovascular lesion.
How often does the “No-Reflow” Phenomenon Occur? 29-44% of reperfused patients 50-80% of reperfused patients with LAD lesion
Does the “No-Reflow” Phenomenon Affect Outcome? YES! Correlates with infarct size, ventricular function and early and late mortality
What is the Mechanism of the “No-Reflow” Phenomenon? Multifactorial: Damage to the microvascular endothelium Wash-in of potent vasoconstrictors Neutrophil activation Platelet activation
A2A/2B Angiogenesis Vasculogenesis ADENOSINE Why Use Adenosine to Prevent the No-Reflow Phenomenon? Reperfusion TxA2, PAF, Ang II, NE, ET-1 Platelets Leukocytes Oxygen Calcium A1/3 A1/3 A2A A2A A2A Oxygen Free Radicals Cellular Calcium Overload MPO Proteases Platelet Aggregation Vasoconstriction Vascular Plugging No Reflow Cell Death