Download
1 / 20
200 likes | 371 Views
‘ Diprifusor’ TCI. Manual control. 十( 4) . TCI 麻醉. 诱导质量. Poor 2.5%. Poor 5.0%. Adequate 22.8%. Adequate 22.5%. Good 74.7%. Good 72.5%. n=79. n =80. The initial infusion rate was higher with `Diprifusor´ TCI (1,200 ml/h) than with manual control

E N D
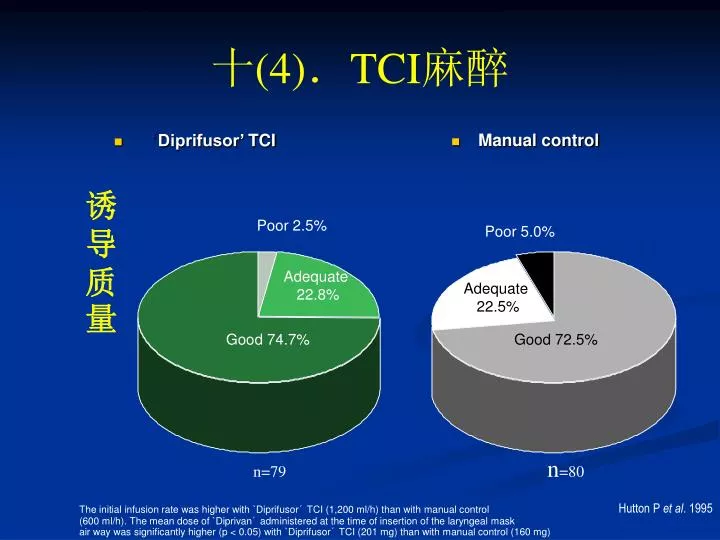
‘Diprifusor’TCI Manual control 十(4).TCI麻醉 诱导质量 Poor 2.5% Poor 5.0% Adequate 22.8% Adequate 22.5% Good 74.7% Good 72.5% n=79 n=80 The initial infusion rate was higher with `Diprifusor´ TCI (1,200 ml/h) than with manual control (600 ml/h). The mean dose of `Diprivan´ administered at the time of insertion of the laryngeal mask air way was significantly higher (p < 0.05) with `Diprifusor´ TCI (201 mg) than with manual control (160 mg) Hutton P et al. 1995
十(4).TCI麻醉 • 麻醉维持 • 靶浓度3~6μg/ml,常规辅助用镇痛药 • 单一异丙酚麻醉,应增加靶浓度 • 推荐维持靶浓度 ASAⅠ-Ⅱ 3.5~5.3μg/ml 、 心脏病人或ASA Ⅲ -Ⅳ 2.8~3.4μg/ml 年龄>55岁 3.5μg/ml • 术中合用其它麻醉药,靶浓度应降低
十(4).TCI麻醉 • 麻醉维持根据手术刺激强弱改变靶浓度 • 靶浓度与效应部位浓度平衡要延迟2~3分钟,尤其老年及ASA Ⅲ或Ⅳ级病人,达到靶浓度需待一定时间,才出现相应的麻醉效应 • 改变靶浓度前,应待目前靶浓度出现相应效应后,再根据麻醉深度进一步调整
十(4).TCI麻醉 • 麻醉维持质量 Manual control ‘Diprifusor’ TCI Poor 3.8% Poor 0% Adequate 22.4% Adequate 27.5% Good 77.6% Good 68.7% n = 76 n = 80 The initial infusion rate was higher with `Diprifusor´ TCI (1,200 ml/h) than with manual control (600 ml/h). The mean dose of `Diprivan´ administered at the time of insertion of the laryngeal mask air way was significantly higher (p < 0.05) with `Diprifusor´ TCI (201 mg) than with manual control (160 mg) Hutton P et al. 1995
十(4).TCI麻醉 NS p = 0.19 30% 28.8% 麻醉维持质量 20%% 19.7% 对切皮运动反应发生率 10% 10% Manual control n = 80 ‘Diprifusor’ TCI n = 76 The mean overall infusion rate during maintenance was significantly greater (p = 0.001) in the ‘Diprifusor’ TCI group (13.2 mg/kg/h) than in the manual control group (8.2 mg/kg/h)
十(4).TCI麻醉 P=0.02 麻醉维持质量 26.2% 11.8% n=80 n=76 The mean overall infusion rate during maintenance was significantly greater (p = 0.001) in the ‘Diprifusor’ TCI group (13.2 mg/kg/h) than in the manual control group (8.2 mg/kg/h) Russell D et al. 1995
十(4).TCI麻醉 50% 麻醉维持质量 10% 3-5doses The mean overall infusion rate during maintenance was significantly greater (p = 0.001) in the‘Diprifusor’ TCI group (13.2 mg/kg/h) than in the manual control group (8.2 mg/kg/h). Settinga higher target concentration with ‘Diprifusor’ TCI results in automatic administration of a bolus 40% 1 – 2 doses 需单次追加用药加深麻醉的比例(%) 25% 0% Manual control n = 80 ‘Diprifusor’ TCI n = 75 Hutton P et al. 1995
十(5). 辅助用药对TCI影响 • 药代学影响 • 阿芬太尼降低异丙酚的分布和清除率,增加异丙酚的血药浓度 • 合并输注阿芬太尼40~80ng/ml时,TCI异丙酚血药浓度增加20% • 异丙酚抑制阿芬太尼氧化代谢的细胞色素P450酶,会增加阿芬太尼的血药浓度 • 通过同样的机制,异丙酚会降低芬太尼和苏芬太尼的代谢
十(5). 辅助用药对TCI影响 • 异丙酚与阿片类药物,药物用量与效应的变化约10~20% • 同一药物药代学在不同个体间的差异达70~80%,药效学个体差异达300~400% • 异丙酚与阿片类药间药代学相互作用引起的小量变化没有明显临床意义
十(5). 辅助用药对TCI影响 • 药效学影响 • 镇静药 异丙酚与咪唑安定或硫喷妥钠的意识消失效应呈现协同作用。术前用咪唑安定可降低异丙酚需要量 咪唑安定(mg) 异丙酚靶浓度 (μg/ml) 诱导成功率(%) 0 3 45 1 3 75 2 3 85 4 3 95
十(5). 辅助用药对TCI影响 • N2O 降低所需异丙酚靶浓度 • 60% N2O,病人切皮反应的异丙酚EC50 14.3μg/ml 3.85μg/ml • 67%N2O,抑制50%病人切皮反应的异丙酚靶浓度6μg/ml 4.5μg/ml。
十(5).辅助用药对TCI影响 • 阿片类镇痛药 • 血浓度250ng/ml阿芬太尼,使异丙酚意识消失的剂量减少50% • 芬太尼血浓度0 0.6ng/ml,50%病人切皮运动反应异丙酚靶浓度16 8μg/ml • 心脏手术,异丙酚靶浓度2 6μg/ml,阿芬太尼的EC50,插管时232 51ng/ml,锯胸骨时103 16ng/ml
十(5).辅助用药对TCI影响 阿片类药物人控输注 芬太尼EC50-EC95阿芬太尼EC50-EC95 苏芬太尼EC50-EC95 瑞美芬太尼EC50-EC95 (1.1-1.6ng/ml)(90-130ng/ml) (0.14-0.20ng/ml) (4.7-8.0ng/ml) 诱导 3μg/kg 25-35μg/kg 0.15-0.25μg/kg 1.5-2μg/kg 30s 静注 30s静注 30s 静注 30s 静注 输注1 1.5-2.5μg/kg/h 50-75μg/kg/h 此后 13-22μg/kg/h 输注30min 输注30min 0.15-0.22μg/kg/h 输注20min 输注2 1.3--2μg/kg/h 此后 此后 输注到150min 30-42.5μg/kg/h 不变 11.5-19μg/kg/h 输注3 此后0.7-1.4μg/kg/h 不变 不变 不变 P-TCI 异丙酚EC50-EC95 异丙酚EC50-EC9 5 异丙酚EC50-EC95 异丙酚EC50-EC95 3.4--5.4μg/ml 3.2-4.4μg/ml 3.3-4.5μg/ml 2.5-2.8μg/ml 恢复时间13-56min 12-37min 13-35min 7-11min 输注方案
十一.TCI在其它方面的应用 • TCI与镇痛 • 最适合用于TCI的药物必须具有在血-脑之间快速平衡的特点 • 阿芬太尼、瑞美芬太尼和苏芬太尼均符合TCI要求,均可用于术中、术后镇痛 • TCI与病人自控镇痛技术相结合实施镇痛,病人通过手控按钮控制TCI药物靶浓度的增减以达到更为理想的镇痛效果
十一.TCI在其它方面的应用 • 氯胺酮难以单独用于麻醉,而其有显著镇痛效应,氯胺酮TCI联合应用其它药物可提供理想的全凭静脉麻醉 • 氯胺酮TCI采用线性开放二室模型,其TCI初始靶浓度200~300ng.ml-1与异丙酚人工输注相结合可提供满意麻醉 • 与异丙酚合并吸入氧化亚氮或异氟醚比,恢复时间无延长,可以替代异丙酚/阿芬太尼作为全凭静脉麻醉
十一.TCI在其它方面的应用 • TCI与自控镇静 • 1997年Irwin等将异丙酚TCI与病人自控镇静结合起来,目前处在研究阶段 • 异丙酚TCI起始靶浓度1μg/ml,病人过连续按两次手动按钮使靶浓度每次增加0.2μg/ml,锁定时间为2分钟,最大允许靶浓度为3μg/ml,如病人6分钟无用药需求,则系统自动将靶浓度降到0.2μg/ml
十一.TCI在其它方面的应用 • 研究结果表明,最适合镇静的异丙酚平均靶浓度为0.8~0.9μg/ml,89%病人愿意再次应用该技术 • 该技术的优点是起效和恢复迅速、根据病人紧张焦虑的程度快速达到病人满意的镇静水平、安全可靠
十一.TCI在其它方面的应用 • TCI与闭路控制麻醉(CLAN) • CLAN ,探测系统自动探测意识水平,其做为反馈信号进入控制系统,由控制系统调节控制输注泵,避免麻醉过浅或过深 • 优点:根据病人的个体差异调节麻醉浓度,克服药代学和药效学的个体间差异;TCI设定的是血液或是效应部位靶浓度,而CLAN设定的是药物效应(靶麻醉深度)
十一.TCI在其它方面的应用 • 在CLAN系统,关键环节是探测麻醉深度 • BIS和AEP是麻醉深度监测的很好指标 • 应用BIS或AEP结合病人的呼吸等作为自动反馈信息,进入控制运算系统,经过运算调节后,再由控制系统控制TCI输注泵调节异丙酚的靶浓度,均取得了满意的麻醉效果,并成功地用于心脏手术的麻醉,实现麻醉自动化
