Download
1 / 30
370 likes | 704 Views
Culture of Safety. HSC Faculty Development Program Niti Armistead, MD FACP October 30 th , 2008. Objectives. Safety from a patient’s perspective Case scenarios from closer to home Science of safety Importance of teamwork and communication Theory to practice: required elements.

E N D
Culture of Safety HSC Faculty Development Program Niti Armistead, MD FACP October 30th, 2008
Objectives • Safety from a patient’s perspective • Case scenarios from closer to home • Science of safety • Importance of teamwork and communication • Theory to practice: required elements
Josie King • Spot for video
Audience Thoughts… • How could this story happen? • Could this happen at any Healthcare facility, including WVUH? • Does organizational “culture” have any role in this issue?
Case Scenario #1 Mr. Jones is a 89 year old man involved in a motor vehicle accident 1 month prior to admission. Over the month, he became progressively confused and lethargic. Head CT by PCP revealed a large left sided subdural hematoma. He was transferred to our facility for further evaluation and treatment.
Case Scenario #1 Upon admission to SICU, patient’s wife was consented for a left twist drill procedure for insertion of a drainage catheter. Dr Smith marked the site while the family was present in the room, while he was talking with them. Family left the room just prior to the procedure. RNs John and Susan were in and out of the room at various times. John was the stat nurse and Susan had another patient assignment. It was shift change and there was a lot of activity in the unit, including many visitors and calls.
Procedure Dr Smith shaved a small spot on the scalp and prepped the area with chloraprep. He placed a drain on the right side of the head. There was no drainage noted. Immediately Dr Smith realized he had placed the drain on the wrong side. He successfully went on to place another drain on the left side. There is a space on the sedation form for the surgical pause and site validation. This space was left blank. Mr. Jones suffered no direct harm from the placement of either drain.
Case Scenario #1 • How could this wrong-site procedure have been prevented?
Science of Safety • Late 1999, Institute of Medicine (IOM) published a report, “To Err is Human: Building a Safer Health System” • Estimated 44,000 to 98,000 deaths from errors • “Equivalent of a jumbo jet crashing each and every day in the U.S.” • Generally not an issue of “bad apples” • Challenge: build a system that catches the inevitable lapses of mortals1 1. Wachter, Shojania. Internal Bleeding. New York, NY: Rugged Land, 2004
The Swiss Cheese Model of Safety Layers of Protection Some holes due to active failures Hazards Other holes due to system design Error Reaches Patient James Reason, Human error
Science of Safety All healthcare encounters All errors All adverse events Preventable adverse events Non-preventable adverse events “near miss” Negligent adverse events Wachter. Understanding Patient Safety, McGraw Hill, NY 2008
Quality versus Safety: for example… • Patient comes in to ED with chest pain. His EKG shows ST elevation, suggesting acute MI. He receives an aspirin and a beta-blocker and taken to the cath lab immediately. In the post procedure time, he receives his metformin and 2 doses of ibuprofen. Patient’s hospital stay is complicated by acute renal failure. • Acute MI quality process measures met? Yes. This is publicly reported and relatively easily measured. • Was his “safety” optimized? No. This is not as easily detected!
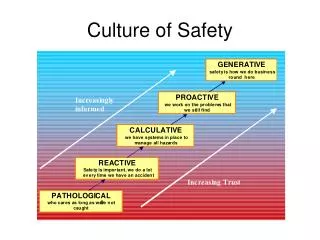
Science of Safety • What does system-focused approach look like? • Technology • Practices • Procedures • Policies • Culture! • Culture: collection of values, beliefs and assumptions that guide members’ behaviors Pronovost et al, Implementing and Validating a Comprehensive Unit-Based Safety program, Journal of Patient Safety. March 2005
Culture of Safety • Culture: “the way we do things around here” Culture Eats Strategy for Lunch
What is a Safe Culture? • “In a safe culture, employees are guided by an organization wide commitment to safety, in which each member upholds their own safety norms and those of their coworkers” • Aviation industry experience supports an association between culture and error management • Teamwork: training diverse crews to dampen steep and unyielding authority gradients • Communication: clear, timely, closed, structured
Preflight briefings and checklists Call-outs Standard procedures Terminology Mitigate error consequences Teamwork Leadership Every defect is learned in real time Production is stopped, Any one can stop the line! (gidoka) Defect is resolved and they learn from the defect (Kaizen) Eliminate waste (muda) Lessons from Other Industries Aviation Industry Toyota Model Anyone can stop the plane Anyone can stop the line Q: has anyone done this in healthcare??? Yes!
Johns Hopkins Experience: Comprehensive Unit-Based Safety Program CUSP 6 steps • Evaluate-AHRQ Survey Tool • Educate on science of safety • Identify defects as a unit • Adopt interventions • Learn from defect and others • Evaluate
Johns Hopkins Experience: Comprehensive Unit-Based Safety Program • Results: • Significant improvement in staffs’ perception about patient safety and safety climate. • Several safety initiatives implemented e.g. ICU daily goals sheet and medication reconciliation • Reduction in ICU nursing turnover • Reduction in ICU length of stay
Teamwork and Communication Attending Surgeon Anesthesiologist Surgical RN CRNA Anesthesia Resident Sexton et al. Errors, stress and teamwork in medicine and aviation, BMJ 2000; 320: 745-749
Teamwork and Communication • All organizations need structure and hierarchies • Taken to extreme, rigid hierarchies lead to frontline staff not “speaking up” • Healthcare is different from aviation: • “team” is very heterogeneous: training, income, status • Come to expect a norm of faulty and incomplete exchange of information • When in doubt, we default to “it must be OK” • Need to change mindset to: “if you’re not sure it’s right, assume it is wrong”
To Err is Human, To Fail is Swiss Cheese? Site marking done while MD distracted No X-ray confirmation Environmental factors Wrong site procedure No time out conducted No one said: “stop! Let’s take a time out!”
Case Scenario #2 Infant was ordered calcium gluconate for low calcium. MD entered order for calcium gluconate 400 mg (100mg/kg) IV push. The peds pharmacist (working on 6th floor) checked the initial order and sent labels to the IV room (4th floor). The IV room tech drew up 40 ml (4000 mg), the dose was checked and sent to the floor. The nurse administering the doses was uncomfortable with the syringe size (60ml) and called the peds pharmacy to ask if the dose was correct. The pharmacist double checked the dose in CHIP and verified the dose was correct. Together they decided to use a syringe pump to administer over 30 minutes rather than IV push. Shortly after, the patient began to experience arrhythmias. The drug was stopped, electrolytes monitored, and patient sent to the PICU.
To Err is Human, To Fail is Swiss Cheese? Physician order doesn’t include concentration Medication prepared in IVR on 4th Floor Order Checked by Peds Pharmacist In 6th floor Satellite Medication administered to pt Nurse calls 6th floor pharmacist and questions dose not volume
Transformation to a Culture of Safety Variations Uniformity Quality focus Financial focus Transparent Restricted Autocratic Team Practice focus Patient centered
Academic Healthcare Experience • “Common qualities shared by top performers included a shared sense of purpose, a hands-on leadership style, accountability systems for quality and safety, a focus on results, and a culture of collaboration” • Keroack at al. Academic Medicine, 2007
What Does Accountability Look Like? • Reasonable performance expectations • Applied fairly, expectations similar for all • Proportional consequences • Appropriate carrots and sticks used to drive system to excellence • “No blame” is dominant front line culture • For innocent slips and mistakes • Clear demarcation of blameworthy acts • E.g. gross incompetence, failure to heed quality/ safety rules, disruptive behavior
Theory to Practice: Required Elements • Teamwork: dampen authority gradients • Leader: do introductions, explicitly welcome input from team members, debriefings after procedures • Communication: standardized format e.g. SBAR • Decreased complexity • Independent checks need to be “independent” • Standardizing processes and practices • Report adverse events, learn from defects
Theory to Practice: Required Elements • Strong leadership and champions • One person’s empowerment is another’s depowerment! • Buy-in from all: this is hard work! • Support the folks who “speak up”: even when everything turns out to have been fine! • Become comfortable with “blame free”, yet holding people accountable, as appropriate.
WVUH “Haunted Hospital” WHO? Everyone - All Ghosts and Goblins! WHAT? Join the fun at our “Haunted Hospital” – Complete with Games, Displays, and GOODIES! WHERE? Ruby – 4th Floor – Conference Rooms 3A/3B WHEN? October 31, 2008 – 12p – 4p November 1, 2008 – 6a – 10a
Conclusion "You've got to be very careful if you don't know where you're going, because you might not get there." Yogi Berra