Download
1 / 1
10 likes | 171 Views
A Head-to-Head Comparison of the Sport Concussion Assessment Tool 2 (SCAT2) and the Military Acute Concussion Evaluation (MACE). Results. Objectives. To evaluate the clinical usefulness of: the Sport Concussion Assessment Tool-Second Edition (SCAT2), in comparison to

E N D
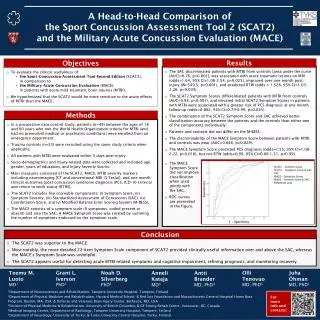
A Head-to-Head Comparison of the Sport Concussion Assessment Tool 2 (SCAT2) and the Military Acute Concussion Evaluation (MACE) Results Objectives • To evaluate the clinical usefulness of: • the Sport Concussion Assessment Tool-Second Edition (SCAT2), • in comparison to • the Military Acute Concussion Evaluation (MACE), • in patients with acute mild traumatic brain injuries (MTBI). • We hypothesized that the SCAT2 would be more sensitive to the acute effects of MTBI than the MACE. • The SAC discriminated patients with MTBI from controls [area under the curve (AUC)=0.76, p<0.001], was associated with acute traumatic lesions on MRI (odds=1.64, 95% CI=1.06-2.54, p=0.025), improved over one month post-injury (W=549.5, p=0.001), and predicted RTW (odds = 1.528, 95% CI=1.03-2.26, p=0.033). • The SCAT2 Symptom Scores differentiated patients with MTBI from controls (AUC=0.84, p<0.001), and elevated initial SCAT2 Symptom Scores in patients with MTBI were associated with a greater risk of PCS diagnosis at one month follow-up (odds=0.882, 95% CI=0.79-0.99, p=0.035). • The combination of the SCAT2 Symptom Score and SAC achieved better classification accuracy between the patients and the controls than either one of the components individually. • Patients and controls did not differ on the M-BESS. • The discriminability of the MACE Symptom Score between patients with MTBI and controls was poor (AUC=0.646, p=0.029). • The MACE Symptom Score predicted PCS diagnosis (odds=1.55, 95% CI=1.08-2.22, p=0.018), but not RTW (odds=0.99, 95% CI=0.66-1.51, p=0.99). • The MACE • Symptom Score • did not improve • classification • when used • jointly with • the SAC. • ROC curves • are presented • in the figure. Methods • In a prospective case-control study, patients (n=49) between the ages of 18 and 60 years who met the World Health Organization criteria for MTBI (and had no premorbid medical or psychiatric conditions) were enrolled from an emergency department. • Trauma controls (n=33) were recruited using the same study criteria when applicable. • All patients with MTBI were evaluated within 5 days post-injury. • Socio-demographics and injury-related data were collected and included age, gender, years of education, and Injury Severity Scores. • Main measures consisted of the SCAT2, MACE, MTBI severity markers including neuroimaging [CT and conventional MRI (3 Tesla)], and one month clinical outcomes [post-concussion syndrome diagnosis (PCS, ICD-10 criteria) and return to work status (RTW)]. • The SCAT2 includes five scoreable components: (i) Symptom Score, (ii) Symptom Severity, (iii) Standardized Assessment of Concussion (SAC), (iv) Coordination Score, and (v) Modified Balance Error Scoring System (M-BESS). • The MACE consists of a symptom scale (9 symptoms, coded present or absent) and also the SAC. A MACE Symptom Score was created by summing the number of symptoms endorsed on the symptom scale. Conclusion • The SCAT2 was superior to the MACE. • Most notably, the more detailed 22-item Symptom Scale component of SCAT2 provided clinically useful information over and above the SAC, whereas the MACE’s Symptom Scale was unhelpful. • The SCAT2 appears useful for detecting acute MTBI-related symptoms and cognitive impairment, refining prognosis, and monitoring recovery. Teemu M. Luoto MD1 Grant L. Iverson PhD2 Noah D. Silverberg PhD3 Olli Tenovuo MD, PhD5 Juha Öhman MD, PhD1 Anneli Kataja MD4 Antti Brander MD, PhD4 1Department of Neurosciences and Rehabilitation, Tampere University Hospital, Tampere, Finland 2Department of Physical Medicine and Rehabilitation, Harvard Medical School; & Red Sox Foundation and Massachusetts General Hospital Home Base Program, Boston, MA, USA; & Defense and Veterans Brain Injury Center, Bethesda, MD, USA 3Division of Physical Medicine & Rehabilitation, University of British Columbia; & GF Strong Rehab Centre, Vancouver, BC, Canada 4Medical Imaging Centre, Department of Radiology, Tampere University Hospital, Tampere, Finland 5Department of Neurology, University of Turku; & Turku University Central Hospital, Turku, Finland For more info and contacts: