Download
1 / 49
590 likes | 1.09k Views
B. C. Isometric force depends on resting muscle length (preload). As in skeletal muscle the force of contraction is very dependent on the geometry of the overlap between the thick and thin filaments. Isometric force depends on resting muscle length (preload).

E N D
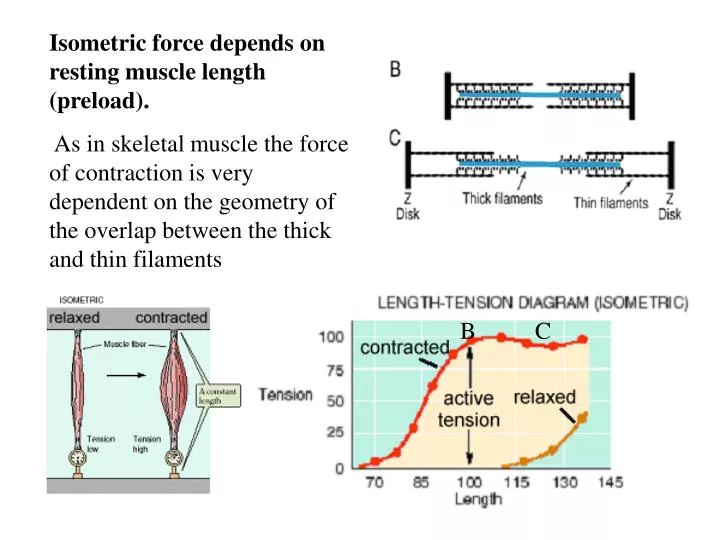
B C Isometric force depends onresting muscle length (preload). As in skeletal muscle the force of contraction is very dependent on the geometry of the overlap between the thick and thin filaments
Isometric force depends onresting muscle length (preload). Starling’s law of the heart: The more the heart is filled during diastole the more forcefully it will contract during systole
The top figure is actually for skeletal muscle because the relaxed tension is still zero at the peak of the contracted curve (Lo). Contrast that to the curve in in the lower panel. The high passive tension opposes over-filling of the ventricle during diastole.
A change in contractility is defined as a change in force of contraction not related to a change in length. A change in contractility can be seen as a shift in the “contracted” curve either up (an increased contractility) or down (a decreased contractility)
Hearts never find themselves beyond Lo due to: • Passive force • Pericardial restraint • Fiber slippage (dilation)
Sympatheic nerve activity is the usual cause of an increased contractility. Heart failure occurs when contractility is pathologically reduced Contractility is hard to measure in patients
Isotonic contraction is where the tension is held constant and the muscle is allowed to shorten The greater the load the slower it shortens If the length is increased at any load the speed of shortening increases The force-velocity curve can be extrapolated to zero force to determine the maximum velocity of shortening,Vmax. Notice that Vmax is the same at all lengths
Vmax should be a length-independent index of contractility. Edmund Sonnenblick Changes in contractility shift the entire curve including the y axis intercept, Vmax
The heart actually contracts in an isotonic manner A tetanized skeletal muscle would contract to here Aortic pressure 3. At this point the ventriclebegins to eject and the contraction becomes isotonic 125 100 2. Isometric contraction as pressure builds 75 stroke Pressure (mmHg) 1. The ventricle is filled volume 50 25 20 40 60 80 100 Volume (ml)
Otto Frank in 1895 appreciated that and tried to use the analysis below to calculate stoke volume of a frog heart. Unfortunately the frog heart starts to relax before the ejection is complete Aortic pressure 3. At this point the ventriclebegins to eject and the contraction becomes isotonic 125 100 2. Isometric contraction as pressure builds 75 stroke Pressure (mmHg) volume 1. The ventricle is passively filled 50 25 20 40 60 80 100 Volume (ml)
In the 1970s Kiichi Sagawa found that, due to their plateaued action potential, canine and human hearts stay activated long enough to reach equilibrium during ejection. 4. Contraction Aortic pressure 3. At this point the ventriclebegins to eject and the contraction becomes isotonic stops here 125 100 2. Isometric contraction as pressure builds 75 stroke Pressure (mmHg) 1. The ventricle is filled volume 50 25 20 40 60 80 100 Volume (ml)
Changing filling pressure changes stroke volume only by changing LVEDV This could be an example of transfusion Lowering LVEDP has the opposite effect
Lowering the aortic pressure causes the ventricle to empty more completely. The stroke volume increases by an amount equal to the fall in LVESV. LVEDV is not affected. This is part of the rationale for afterload lowering therapy Raising aortic pressure has the opposite effect
Increasing contractility decreases LVESV and thus increases stroke volume. LVEDV is not affected. Heart failure has the opposite effect
There are only three ways that the body can alter stroke volume from minute-to-minute: • Filling pressure (preload) • Aortic pressure (afterload) • Contractility
Actually the heart beat is Auxotonic i.e the load changes during shortening For our analysis isotonic is a close approximation
Decreasing the diastolic compliance decreases LVEDV and stroke volume but has no effect on LVESV Decreased compliance is a serious compli-cation for hearts with concentric hypertrophy
Decreases diastolic compliance Pressure overload causes concentric hypertrophy where the ventricle remodels inwardly to a low lumen volume and a thick wall. Caused by hypertension or outflow track obstruction.
Caused byregurgitant aortic valve or AV fistulas. Volume overload leads to eccentric hypertrophy. The heart remodels outwardly to give a large lumen diameter but a near normal wall thickness. Increases diastolic compliance
Changes in compliance occur only in disease and are not a physiological regulator • Wall thickening or thinning • Delayed or incomplete relaxation
1960’s Sarnoff’s ventricular function curve.
Three factors control the stroke volume: filling pressure, aortic pressure and contractility. So how can we control for the former two?
By plotting the stroke work against filling pressure any change in filling pressure is accounted for.
Using stroke work instead of stroke volume corrects for changes in aortic pressure.
Notice that stroke volume and aortic pressure change in a reciprocal manner. Stroke Work = AOP x SV As AOP goes up SV naturally goes down so their product remains relatively constant. Stroke work should be independent of any change in blood pressure.
Changes in contractility change stroke volume. Changes in aortic pressure also change stroke volume. Since aortic pressure changes reciprocally with aortic pressure their product (stroke work) is independent of aortic pressure
Disadvantages of the cardiac performance curve method 1. Highly invasive 2. Cannot make comparisons between patients (not a useful clinical test)
How can we measure contractility in the patient? Ejection fraction = (LVEDV-LVESV) / LVEDV The fraction of the ventricular contents at end diastole that is ejected.
How can we measure contractility in the patient? Ejection fraction = (LVEDV-LVESV) / LVEDV • Can be easily measured But…. • Affected by contractility • Affected by preload • Affected by afterload • Affected by compliance
Thus, dP/dt of the ventricular pressure increases with contractility Changes in contractility shift the entire force-velocity curve. At any afterload increasing contractility increases velocity of shortening.
Vmax The maximum velocity of shortening Vmax as calculated from the force velocity curve is independent of length and a good index of contractility. Vmax in an intact heart can be estimated from the ventricular pressure with: dP/dt. P
Vmax Unfortunately, Vmax seems to measure the contractility of the best muscle in the heart and is a poor index in regional dysfunction.
The heart appears to vary its elasticity from very elastic in diastole to very stiff in systole. slope =Emax Pressure Elasticity = ΔV/ΔP Stiffness = Δ P /ΔV Volume Vo
The maximum stiffness Emax occurs during systole. Emax and Vo (volume at zero pressure) describe the ventricle. slope =Emax Pressure Volume Vo
A device called the conductance catheter allows instantaneous measurement of ventricular volume and pressure so that an ejection loop can be viewed in real time in a patient. By varying aortic pressure several end-systolic pressure-volume points can be measured.
By fitting a straight line to the ESPVR, Emax and Vo cal be calculated
The area within the ejection loop is proportional to the mechanical work done by the heart (external work).
The external work correlates poorly with the oxygen consumption (metabolic energy) of the heart.
If the triangle to the left of the ejection loop is added to the area of the ejection loop, the correlation with oxygen consumption on a per beat basis is almost perfect. It can be shown that the triangle correlates with internal work during the isovolumetric phase of contraction.
Increased blood pressure may cause less external work but will always increase oxygen consumption. Elevated blood pressure puts a high metabolic load on the heart.
Decreasing blood pressure will always decrease oxygen consumption.
A patient receives a drug that increases aortic pressure and decreases end diastolic pressure. What did the drug do?
What are the pros and cons of the ejection fraction as an estimate of contractility?