Download
1 / 44
460 likes | 721 Views
INJURIES TO THE HEAD, NECK & SPINE. HEAD INJURIES ARE AMONG THE MOST SERIOUS SINCE THEY CAN CAUSE LIFE-LONG COMPLICATIONS & DEATH. YOUR ROLE AS FIRST TRAINED RESCURER ON SCENE IS CRITICAL. THESE INJURIES ARE A LIFE-THREAT SINCE THEY COMPROMISE THE UPPER AIRWAY. HEAD INJURIES.

E N D
INJURIES TO THE HEAD, NECK & SPINE HEAD INJURIES ARE AMONG THE MOST SERIOUS SINCE THEY CAN CAUSE LIFE-LONG COMPLICATIONS & DEATH. YOUR ROLE AS FIRST TRAINED RESCURER ON SCENE IS CRITICAL. THESE INJURIES ARE A LIFE-THREAT SINCE THEY COMPROMISE THE UPPER AIRWAY.
HEAD INJURIES CAN BE OPEN OR CLOSED, EITHER WAY, THERE CAN BE SERIOUS INJURY TO THE BRAIN. THE SKULL HOLDS BLOOD, CEREBROSPINAL FLUID & BRAIN TISSUE. THE VOLUME OF EACH CAN VARY, BUT THE TOTAL VOLUME CAN’T SINCE THE SKULLS CAPACITY IS LIMITED.
SIGNS & SYMPTOMS • ALTERED MENTAL STATUS • IRREGULAR BREATHING • OPEN WOUNDS TO THE SCALP • PENETRATING HEAD WOUND • SOFTNESS OR DEPRESSION IN SKULL • BLOOD &/OR CEREBROSPINAL FLUID LEAKING FROM EARS &/OR MOUTH
FACIAL BRUISES • BRUSING AROUND EYES (RACCOON EYES) • BRUSING BEHIND EARS (BATTLE’S SIGN) • ABNORMAL P M S • VERY SEVERE HEADACHE, CAN BE DISABLING OR APPEARS SUDDENLY • NAUSEA, VOMITING
UNEQUAL PUPIL SIZE &/OR LITTLE OR NO REACTION WITH ALTERED MENTAL STATUS • SEIZURE ACTIVITY
GENERAL EMERGENCY CARE IF YOU HAVE HEAD INJURIES, BE SURE TO ACTIVATE E M S, & ALWAYS STABLIZE CERVICAL SPINE. BE SURE TO TAKE B S I PRECAUTIONS SINCE THERE IS A GOOD POSSIBILITY OF BLOOD &/OR CEREBROSPINAL FLUID.
GENERAL EMERGENCY CARE • A B C’s & O2, MAKE AIRWAY TOP PRIORITY WITH HIGH FLOW O2 • CONTROL BLEEDING & DRESS OPEN WOUNDS • APPLY C-COLLAR • CLOSELY MONITOR VITALS • CALM & REASSURE PATIENT
SYMPTOMS & SIGNS SKULL FRACTURE • SKULL DAMAGE VISIBLE THROUGH SCALP LACERATIONS • SKULL OR FACIAL DEFORMITIES • SWELLING & PAIN AT INJURY SITE • CLEAR OR PINKISH FLUID FROM NOSE, EARS, MOUTH OR HEAD WOUND
UNUSUAL PUPIL SIZE & SUNKEN EYE • PURPLISH BRUISING AROUND EYES (RACCOON EYES) • PURPLISH BRUISING BEHIND EARS (BATTLE’S SIGN)
BRAIN INJURIES SIGNS & SYMPTOMS • CHANGES IN MENTAL STATUS • PARALYSIS OR FLACCIDITY USUALLY ONLY ON ONE SIDE OF BODY • UNEQUAL FACIAL MOVEMENT, SQUINTING, DROOPING, UNEQUAL &/OR UNRESPONSIVE PUPILS & VISION DISTURBANCES IN ONE OR BOTH EYES
RINGING,LOSS OF HEARING IN ONE OR BOTH EARS • RIGIDITY OF ALL LIMBS • SLOW, STRONG HEART BEAT THAT BECOMES RAPID & WEAK • HIGH BP WITH SLOW PLUSE • RAPID, LABORED BREATHING & DISTURBED BREATHING PATTERN • VOMITING • INCONTINENCE
CONCUSSIONSIGNS & SYMPTOMS • MOMENTARY CONFUSION OR CAN LAST FOR SEVERAL MINUTES • NO RECALL OF THE TIME BEFORE & AFTER INJURY • REPEATEDLY ASKED WHAT HAPPENED • IRRITABLE, UNCOOPRERATIVE, COMBATIVE & VERBALLY ABUSIVE
INABILITY TO ANSWER QUESTIONS OR OBEY COMMANDS • PERSISTENT VOMITING • INCONTINENCE • RESTLESSNESS • SEIZURES • BRIEF LOSS OF CONSCIOUSNESS
PENETRATING WOUND • DO NOT TRY TO RMOVE IMPAILED OBJECT • STABILIZE WITH SOFT BULKY DRESSINGS • DRESS REST OF WOUNDS • NEVER APPLY PRESSURE
NECK INJURIES COMMON CAUSES ARE HANGING (ATTEMPTED SUICIDE), IMPACT WITH STEERING WHEEL & CLOTHSLINED ON WIRE. LARGE INJURIES MAY INVOLVE MAJOR BLOOD VESSELS WHICH CAN PRODUCE FATAL BLEEDING. THERE ALSO MAY BE AN AIR EMBOLISM.
SIGNS & SYMPTOMS • OBVIOUS LACERATIONS & OTHER WOUNDS • DEFORMITIES OR DEPRESSIONS • OBVIOUS SWELLING, CAN BE IN FACE OR CHEST • DIFFICULTY SPEAKING OR LOSS OF VOICE
AIRWAY OBSTRUCTION • CRACKLING SENSATIONS UNDER THE SKIN/AIR LEAKING INTO SOFT TISSUES (SUBCUTANEOUS EMPHYSEMA)
BLEEDING FROM NECK APPLY SLIGHT TO MODERATE PRESSURE USING AN OCCLUSIVE DRESSING & THEN TAPEING EDGES DOWN TO FORM AN AIR-TIGHT SEAL. ADD A BULKY DRESSING OVER OCCLUSIVE. NEVER APPLY PRESSURE TO BOTH SIDES OF THE NECK AT THE SAME TIME.
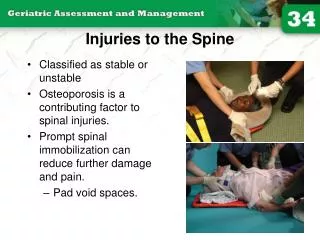
INJURIES TO THE SPINE FROM THE TIME YOU FIRST ARRIVE ON SCENE YOUR FIRST CONSIDERATION IS SPINAL INJURY & TO TAKE PROPER ACTION. REMEMBER, IF YOU FAIL TO ACCOMPLISH THIS TASK YOU CAN CONDEM A PATIENT TO LIFE IN A WHEELCHAIR OR EVEN DEATH.
THE SPINE IS MADE UP OF 33 BONES STACKED ON TOP OF EACH OTHER. THESE VERTEBRAEARTICULATE, OR FIT & MOVE TOGETHER SO THAT WE BEND, TURN & FLEX.
REGIONS OF THE SPINE • CERVICAL • THORACIC • LUMBAR • SACRAL • COCCYGEAL
CERVICAL SPINE • STARTS AT BASE OF SKULL • CONSISTS OF 7 VERTEBRAE • HOUSES SPINAL CORD • SUPPORTS WEIGHT OF HEAD • VERY VULNERABLE TO INJURY
THORACIC SPINE • SUPPORTED BY RIB CAGE • CONSISTS OF 12 VERTEBRAE • ONE VERTEBRAE FOR EACH PAIR OF RIBS • LESS FREQUENTLY INJURED
LUMBAR SPINE • CONSISTS OF 5 VERTEBRAE • CARRIES MOST OF BODIES WEIGHT • LARGEST VERTEBRAE • VERY VULNERABLE TO INJURY
SACRAL SPINE • CONSISTS OF 5 VERTEBRAE • ALL 5 ARE FUSED SO THEY DO NOT BEND EASILY
COCCYGEAL SPINE • CONSISTS OF 4 VERTEBRAE • ALL 4 ARE FUSED • IN CONJUNCTION WITH THE SACRAL SPINE, THEY FORM THE POSTERIOR PORTION OF THE PELVIS
EMERGENCIES WITH HIGH % OF SPINE INJURIES • M V A’s • MOTORCYCLE ACCIDENTS • PEDESTRIAN-CAR ACCIDENTS • FALLS • DIVING ACCIDENTS • HANGINGS • BLUNT TRAUMA
PENETRATING TRAUMA TO THE HEAD, NECK OR TORSO • GUNSHOT WOUNDS • SPEED SPORTS, ROLLER BLADING, BICYCLING, SKIING, SURFING OR SLEDDING • ANY UNRESPONSIVE TRAUMA PATIENT
IF THE MECHANISM OF INJURY SUGGESTS IT, ALWAYS PROCEED AS IF THERE IS A SPINAL INJURY. EVEN IF THE PATIENT SAYS HE IS NOT INJURED, HAS NO PAIN IN SPINAL AREA, CAN WALK, MOVE ARMS & HAS FEELING SENSATION,YOUCANNOT RULE OUT SPINAL INJURY.
SIGNS & SYMPTOMS • RESPIRATORY DISTRESS • TENDERNESS AT INJURY SITE • PAIN ALONG SPINAL COLUMN WITH MOVEMENT(do not move patient or ask patient to move to check for pain) • CONSTANT/INTERMITTENT PAIN WITHOUT MOVEMENT ALONG SPINAL COLUMN OR IN LOWER LEGS
OBVIOUS SPINAL DEFORMITY(this is rare) • SOFT-TISSUE INJURIES TO HEAD, NECK, SHOULDERS, BACK, ABDOMEN OR LEGS • NUMBNESS, WEAKNESS OR TINGLING IN ARMS &/OR LEGS • LOSS OF SENSATION OR PARALYSIS IN UPPER OR LOWER EXTREMITIES OR BELOW INJURY SITE
INCONTINENCE OR LOSS OF BOWEL OR BLADDER CONTROL • PRIAPISM OR A CONSTANT ERECTION OF THE PENIS (a classic sign of cervical spine injury)
ASSESSMENT OF SPINAL INJURIES • SCENE SIZE-UP • STABILIZE HEAD & NECK • A B C’s (be sure to use jaw-thrust to open airway) • HIGH FLOW O2 • ASSESS P M S • MAINTAIN STABILIZATION & MONITOR AIRWAY & BREATHING
IMMOBILIZATION TECHNIQUES • CERVICAL IMMOBILIZATION • LONG BOARD IMMOBILIZATION • RAPID EXTRCATION • HELMET REMOVAL
CERVICAL IMMOBILIZATION • SLIDE POSTERIOR PORTION OF THE COLLAR THROUGH THE GAP UNDER THE PATIENT’S NECK • FLIP ANTERIOR PORTION OVER THE CHIN • SECURE WITH VELCRO STRAP, BE CAREFUL NOT TO PULL TOO HARD SINCE IT CAN TWIST THE HEAD
CHECK P M S BEFORE & AFTER APPLYING COLLAR • REMEMBER, THE COLLAR ONLY SUPPLIES 50% STABILIZATION, YOU MUST SUPPLY 50% MANUALLY
LONG BOARD IMMOBILIZATION ONCE YOU HAVE APPLIED A CERVICAL COLLAR, YOU NEED TO IMMOBILIZE THE PATIENT ON A LONG BOARD. YOU NEED TO ROLL THE PATIENT, PLACE THE BOARD UNDER HIM, THEN ROLL HIM BACK ON THE BOARD. THIS IS CALLED A LOG ROLL. REMEMBER TO CHECKP M S BEFORE & AFTER.
LOG ROLL • POSITION PATIENT • CHECK P M S • POSITION RESCUERS • PERSON AT HEAD IS IN CHARGE, THEY WILL GIVE ALL COMMANDS FOR MOVEMENT • ROLL PATIENT ON SIGNAL FROM HEAD PERSON
POSITION THE BOARD • ROLL PATIENT BACK DOWN ON BOARD ON SIGNAL FROM HEAD PERSON • REASSESS P M S
SECURING PATIENT TO LONG BOARD • IMMOBILIZE TORSO, HEAD & LEGS IN THAT ORDER • STRAPS SHOULD BE AT NIPPLES, NAVEL & KNEES(Above & Below) • WITHDRAW MANUAL STABILIZATION • REASSESS P M S
WHEN IS RAPID EXTRACATION NEEDED • WHEN SCENE IS NOT SAFE, THREAT OF FIRE OR EXPLOSION • LIFE-SAVING CARE CANNOT BE GIVEN BECAUSE OF PATIENT’S LOCATION OR POSITION • INABILITY TO GAIN ACCESS TO OTHER PATIENTS WHO NEED LIFE-SAVING CARE
RAPID EXTRICATION • STABILIZE CERVICAL SPINE • APPLY CERVICAL COLLAR • ROTATE PATIENT • PLACE LONG BOARD IN LINE WITH PATIENT • LOWER PATIENT & POSITION ON BOARD • SECURE PATIENT TO BOARD
HELMET REMOVAL IN GENERAL, IF THE PATIENT CAN BE ASSESSED PROPERLY & THE AIRWAY MAINTAINED, LEAVE THE HELMET IN PLACE. NEVER TRY TO REMOVE A HELMET ALONE, WAIT FOR HELP.
HELMET REMOVAL STEPS • STABLIZE HELMET, ONCE STABILIZED DO NOT STOP STABILIZATION • LOOSEN CHIN STRAP • TRANSFER STABILIZATION • REMOVE HELMET HALF WAY • COMPLETE REMOVAL • APPLY CERVICAL COLLAR • IMMOBILIZE ON LONG BOARD