Download
1 / 40
400 likes | 551 Views
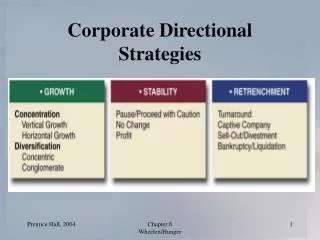
Reducing HAIs: Effective Change Strategies . Anthony Harris MD, MPH Professor Acting Medical Director of Infection Control Head Division of Genomic Epidemiology and Clinical Outcomes University of Maryland School of Medicine. Who am I: what am I and what am I not qualified to talk about?.

E N D
Reducing HAIs: Effective Change Strategies Anthony Harris MD, MPH Professor Acting Medical Director of Infection Control Head Division of Genomic Epidemiology and Clinical Outcomes University of Maryland School of Medicine
Who am I: what am I and what am I not qualified to talk about?
Outline of talk • Discussion of important healthcare-associated infection (HAIs) • Science of how to decrease HAIs • Epidemiological issues of HAIs research • Barriers to implementation and maintenance • Illustrative examples
Outline of talk • Discussion of important healthcare-associated infection (HAIs) • Science of how to decrease HAIs • Epidemiological issues of HAI research • Barriers to implementation and maintenance • Illustrative examples
HAIs • Central-line associated bacteremias • Ventilator-associated pneumonia • Surgical-site infection • Catheter-associated urinary tract infection
1 of every 10-20 patients hospitalized in the United States develops a healthcare-associated infection Importance of HAIs
Importance of HAIs • The US Centers for Disease Control and Prevention estimates that nearly 2 million patients (5%-10% of hospitalized patients) experience an HAI each year • These infections lead to almost 100,000 deaths and $28-$33 billion in extra costs.
Cost of HAIs Eber MR, Arch Intern Med. 2010;170:347
Outline of talk • Discussion of important healthcare-associated infection (HAIs) • Science of how to decrease HAIs • Epidemiological issues of HAI research • Barriers to implementation and maintenance • Illustrative examples
I am a hospital epidemiologist, infection preventionist, or hospital administrator with an HAI problem what literature should I look at that shows what interventions may work?
Infection Prevention Goals Improving Health and Patient Safety by reducing risk of Infection
SHEA guidelines • Centers for Disease Control and Prevention • HICPAC guidelines • IDSA • APIC • HHS
SHEA guidelines • To assist acute care hospitals in focusing and prioritizing efforts to implement evidence-based practices for prevention of HAIs, the Society for Healthcare Epidemiology of America and the Infectious Diseases Society of America Standards and Practice Guidelines Committee appointed a task force to create a concise compendium of recommendations for the prevention of common HAIs http://www.sheaonline.org/about/compendium.cfm
CLBSI 14
CLABSI: Effective interventions • At insertion • Use a catheter checklist to ensure adherence to infection prevention practices at the time of central venous catheter insertion • Perform hand hygiene before catheter insertion or manipulation • Avoid the femoral vein • Use an all-inclusive catheter cart or kit • Use maximal sterile barrier precautions during central venous catheter insertion • Use a chlorhexidine-based antiseptic for skin preparation
CLABSI: Effective interventions • After insertion • Disinfect catheter hubs, needleless connectors, and injection ports before accessing the catheter • Remove nonessential catheters
Effective interventions in difficult situations • Bathe ICU patients with a chlorhexidine preparation on a daily basis • Use antimicrobial-impregnated central venous catheters • Use chlorhexidine-containing sponge dressings for central venous catheters • Use antimicrobial locks for central venous catheters
VAP: Effective interventions • Implement policies and practices for disinfection, sterilization, and maintenance of respiratory equipment • Ensure that all patients are maintained in a semi-recumbent position • Perform regular antiseptic oral care in accordance with product guidelines • Provide easy access to noninvasive ventilation equipment and use weaning protocols
UTI: Effective interventions • Provide and implement written guidelines for catheter use, insertion, and maintenance • Ensure that only trained personnel insert urinary catheters • Ensure that supplies necessary for aseptic-technique catheter insertion are available • Implement a system for documenting: indications for catheter insertion, date and time of catheter insertion, individual who inserted catheter, and date and time of catheter removal
SSI: Effective interventions • Administer antimicrobial prophylaxis • Do not remove hair at the operative site unless the presence of hair will interfere with the operation • Do not use razors • Control blood glucose level during the immediate postoperative period for patients undergoing cardiac surgery • Measure and provide feedback to providers on the rates of compliance with the above process measures
Outline of talk • Discussion of important healthcare-associated infection (HAIs) • Science of how to decrease HAIs • Epidemiological issues of HAI research • Barriers to implementation and maintenance • Illustrative examples
Epidemiological barriers • Too few randomized clinical trials • Few to no cluster randomized trials in infection control • Sub-optimal quasi experimental studies
Definition • Q: What is a quasi-experimental study? • A: Study that aims to evaluate interventions but does not utilize a randomized control group
Textbooks Shadish et al. Experimental and Quasi-experimental Designs. Houghton Mifflin Co; 2001. Cook and Campbell. Quasi-experimentation: Design and Analysis Issues for Field Settings. Houghton Mifflin Co; 1979.
Types of QE Studies • (A) Quasi-experimental designs without control groups • (B) Quasi-experimental designs that use control groups but no pretest • (C) Quasi-experimental designs that use control groups and pretests • (D) Interrupted time-series designs Harris AD. The use and interpretation of quasi-experimental studies in infectious diseases. Clin Infect Dis. 38:1586-91. 2004
Hierarchy of QE Designs A. Quasi-experimental designs without control groups • The one-group pretest-posttest design:O1 X O2 • The one-group pretest-posttest design using a double pretest:O1 O2 X O3 • The one-group pretest-posttest design using a nonequivalent dependent variable: (O1a, O1b) X (O2a, O2b) • The removed-treatment design:O1 X O2 O3 removeX O4 • The repeated-treatment design:O1 X O2 removeX O3 X O4 O = observational measurement; X = intervention under study. Time moves from left to right.
Systematic Review ID Literature (cont) • 73 articles used quasi-experimental designs in infection control and/or antibiotic resistance studies in 4 journals over a 2 year period • Few studies used higher-level quasi-experimental design • Only 16% used a control group Harris et al. Clin Infect Dis. 2005;41:77-82.
Future Quasi-experimental Studies Should Include… • Use of standard nomenclature • Choice of “higher level” studies if possible • Add control group, multiple measurements • Discussion of why the specific study design and analysis was chosen • Discussion of particular study limitations • Collaboration with statisticians to improve analysis Stone SP, The Orion Statement J Antimicrob Chemother. 2007 May;59:833
Outline of talk • Discussion of important healthcare-associated infection (HAIs) • Science of how to decrease HAIS • Epidemiological issues of HAI research • Barriers to implementation and maintenance • Illustrative examples
In the day-to-day world certain issues arise: • How do you sustain an intervention? • How do you get ground-level buy in? • How do you deal with the powerful naysayers? • What logistical issues arise? • How do you stay on top of all the logistical issues?
Health Behavior and Health Education Karen Glanz, Barbara K. Rimer and K. Viswanath 3rd edition 2002 Resources for affecting health behavior
Resources for affecting health behavior: Positive deviance • In healthcare-associated infections, leaders such as Dr. B Doebbeling are using techniques such as integrated lean and positive deviance • Marsh et. al, The Power of Positive Deviance BMJ. 2004:13;329:1177.
Six sigma • Assessing the evidence of six sigma and lean in the health care industry • DelliFraine JL Qual Manag Health Care. 2010;19:211.
Illustrative example: Hand Hygiene • Literature has consistently shown hand hygiene levels to be below 60% • Numerous interventions work but only temporarily • Yet, JCAHO during their audits aims for 100% levels
Illustrative example: CLABSI checklists • Fear of places in reporting what happens at the ground level • Difficulty empowering nurses • Difficulty in getting CEO/CMO buy-in • Powerful naysayers in the ICU
“As a Nurse, … I Can Prevent HAIs!
Illustrative example: CLABSI • This all leads to • Signing the checklist and not being there to supervise • Checklist indicating that all was done properly when many aspects were not • Constant need to monitor what is going right and what is going wrong
Conclusions • HAIs can be reduced • Level of science needs to be improved to determine which interventions are optimal • Maintenance and sustainability of successful interventions is a difficult process