Download
1 / 68
690 likes | 710 Views
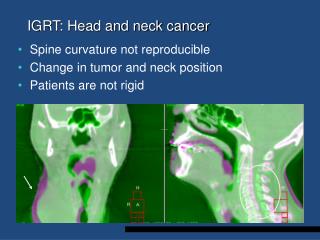
History and evolution of quality of life in head and neck cancer. Hisham Mehanna Consultant Head Neck Surgeon University Hospitals Coventry Warwickshire & Heart of England Foundation Trust, Birmingham Hon Senior Lecturer, Warwick Med School, UK. Leroy A Schall, 1954.

E N D
History and evolution of quality of life in head and neck cancer Hisham Mehanna Consultant Head Neck Surgeon University Hospitals Coventry Warwickshire & Heart of England Foundation Trust, Birmingham Hon Senior Lecturer, Warwick Med School, UK
Leroy A Schall, 1954. “It is hard properly to evaluate human suffering: the blind say they would rather be blind than deaf; whilst the patient without a voice considers himself fortunate that he is neither blind nor deaf.”
Overview Definitions Characteristics of QoL History of QoL concept Evolution of QoL in HNC Evolution of studies QoL Questionnaires Current state Future uses Summary
Why is QoL important? • Impact of HNC on • daily functions • disfigurement • HNC patient requirements over and above other cancer pts • Several different treatments with equivalent survival rates
Definitions Health-related Quality of life Gap between where patient is (experience) and where they would like to be (expectations) and perceived and actual goals Calman 1987
Mehanna’s Health related QoL Reality Expectation
Health-related QoL = one’s personal, subjective assessment of general well-being which can be regarded as a composite scale involving many contributing domains. Characteristics of QoL Concept • self-reported • subjective • multi-dimensional • changes over time
Tenants of QoL assessment • Global vs component measures • Important domains • physical function • psychological state • social interaction • somatic sensation / symptoms • Generic vs disease specific QoL • Domain - specific questionnaires
Voltaire 1694-1761 ‘doctors are men who prescribe medicine of which they know little, to cure diseases of which they know less, in human beings, of which they know nothing’
Jessett 1886 On maxillary cancer “... the only hope we have of permanently benefiting the patient suffering from this disease is by free and extensive operations, i.e., thoroughly removing the whole of the cancerous tissues and getting to healthy structures.”
Nahum and Golden 1963 ‘Since the common tendency of the physician and family is to be sympathetic toward the post-laryngectomy patient, it is often necessary to lean a bit in the opposite direction and to deal with the situation lightly’.’
Watson 1966 on breast cancer • ‘an affliction of an easily disposable utilitarian appendage’ • ‘…evidence (of psychological trauma) will usually have been produced by the enquiry (into QoL) rather than disclosed by it. The adoption of a casual attitude by the doctor before the operation and throughout the follow-up examinations will go a long way towards eliminating these untoward and unnecessary occurrences’
Hippocrates c. 460-377 BC Some patients though conscious that their condition is perilous, recover their health simply through their contentment with the goodness of the physician
M.R. Ewing & Hayes Martin, 1952 "in deciding the method of treatment we should not, in our eagerness to achieve cure, lightly disregard the crippling that may result from our surgical endeavours".
Ormerod, 1954 described explaining to a patient what is entailed in a laryngectomy, including counselling by a speech therapist and interviews with previous patients.
Hospice movement, 1960s pioneered by : Cecily Saunders in Britain, and Elizabeth Kubler-Ross in the U.S.A.
Heckscher 1960 Essay to Dwight Eisenhower’s Commission on National Goals ‘…a society which puts a value on the quality of its national life will want to act resolutely…’
Medline keyword 1977 • 1978-80 200 papers • 1987 400 papers • 1993 1,255 papers • 1996 3,130 papers • 1999 4,564 papers • 2002 6,288 papers • 2005 9,450 papers
Karnofsky 1948 lung cancer • Functional status scale • Subjective Improvement scale • Three category scale
Priestman & Baum 1976 • 10 item questionnaire • Breast cancer Modern approach to QoL measurement
HNC QoL – the start • Non-validated, unidimensional measures • Cross-sectional studies • Descriptive then quantitative • Pitkin 1953 – first study, 61 Lx pts, psychosocial • 1980s-90s prospective studies, validated questionnaires • Johnston 1982 • Browman, 1993 – first RCT • Hassan & Weymuller 1993 • Morton 1995
Guidelines on devt of QLQ Kirshner and Guyatt 1985
Current state • Longitudinal studies • Many (validated) questionnaires • Routine use of QoL • Research outcomes • Clinical outcomes
Current state • Longitudinal studies
Longitudinal studies Morton , 1995,2003, Hammerlid 2001, List 1996, Terrell 1999, Weymuller 2000, Rogers 1999
Deterioration in the long-term (10 year) quality of life of head and neck cancer survivors Mehanna and Morton, Clin Otol 2006
Results : Long-term QL Mehanna and Morton 2006 Life Satisfaction Score 10 yr survivors 65 n = 200 Full cohort 60 “something happened” p < 0.001 55 n: 124 n: 184 n: 43 0 3m 1y 2y 10y
Current state • Longitudinal studies • Many (validated) questionnaires
"choosing an instrument is an exercise in trade offs" Moinpour et al ,1989
“Choosing which instrument to use poses a challenge for investigators of QOL in head and neck cancer...No one instrument is ideal for all purposes.” Ringash and Bezjak, 2001
Lesson 1 Avoid obscure questionnaires
Current state • Longitudinal studies • Many (validated) questionnaires • Routine use of QoL • Research outcomes • Clinical outcomes?
QoL use in UK 29% BAHNO respondents used quality of life questionnaire (QLQ) Major impediments: lack of resource and time Kanatas & Rogers, Ann R Coll Surg Engl, 2004
QoL use in Australasia 34% had ever used QLQ Physicians > surgeons: clinical trials 13% current users only 1.5% routine clinical practice Mehanna and Morton, JLO, 2006
Time consuming/ lack resource No clinical value Don’t know how to use info Patient don’t like it Aus-NZUK 34% 57% 34% 16% 11% 13% 7% 10% Impediments to use Most are clinician based reasons
Lesson 2 K.I.S.S. - Keep it simple for surgeons
Current uses • Providing patients with better information on course of disease and prognosis. • Assessing new and existing treatments and techniques. • Weighing up treatment options and aiding patient decision making.
Better information • Most patients want information Semple 2002 • Better info improves QoL and satisfaction, decreases anxiety • Most HNC pts want more info from MDT Zeigler, 2004
Current uses • Providing patients with better information on course of disease and prognosis. • Assessing new and existing treatments and techniques.
Assessing techniques • New Therapies • T2 larynx – laser vs RT • T3 tonsil tumour – surgery vs CRT • Techniques • Oropharyngeal surgery – primary closure better swallowing than flap • IMRT for parotid sparing - PARSPORT
Current uses • Providing patients with better information on course of disease and prognosis. • Assessing new and existing treatments and techniques. • Weighing up treatment options and aiding patient decision making.