Download

1 / 38
380 likes | 401 Views
Facilitating a global healthcare team collaboration to enhance patient safety in congenital heart surgery for children in developing countries. Tailored quality improvement strategies, telemedicine platform, and nurse empowerment to reduce mortality and complications. Modules cover key drivers to enhance surgical safety and reduce infections.

E N D
International Quality Improvement Collaborative for Congenital Heart Surgery
Vision Facilitate a collaborative of healthcare teams from around the world creating a culture of patient safety & quality for children receiving congenital heart surgery in developing countries
Mission Our mission is to reduce mortality and major complications for children undergoing congenital heart surgery.
Objective Create tailored quality improvement strategies to reduce mortality and major complications for developing world programs. Employ a telemedicine platform to facilitate distance learning, dialogue, disseminate knowledge & skills.
Drivers of Mortality Team-based practice through nurse empowerment Reduce surgical site infections and bacterial sepsis Safe perioperative practices
Key Driver Diagram Change Strategies Key Drivers Aim Utilize a surgical safety checklist to prompt and document evidence-based process measures (i.e. antibiotics given within 60 minutes of surgical incision) Safe Operative Practice Focus on hand hygiene for ALL clinical personnel in contact with patient care. Reduction In 30 day mortality associated with congenital heart surgery Reduce Surgical SiteInfections & Bacterial Sepsis Empowering nurses Evidence-based nursing practice Scripting nurses in ward and ICU on how to give reports Accurate 24hr total patient intakes and outputs Accurate daily recording of patient weight Effective Communication-SBAR Team-based Practice
Learning Modules Learning Module I: Team-based practice and nurse empowerment Learning Module II: Reducing surgical site infection and bacterial sepsis Learning Module III: Safe perioperative practice
Learning Modules Contain quality improvement strategies for each of the 3 drivers that impact mortality addressed during the webinars. Each module contains a series of 3 educational sessions. Sessions advance from beginning, intermediate, and advance-level of learning & acquisition of skills.
Timeline for Webcasts The color of each Learning Module corresponds to the date the that topic will be presented during that month’s webcast. For example, Team-based Practice will be the topic 2/17, 5/19, and 8/18.
Data Entry Map Founding Sites New Sites
Cumulative Site Participation *Graph captures only sites that have entered > 10 patients into the IQIC Database.
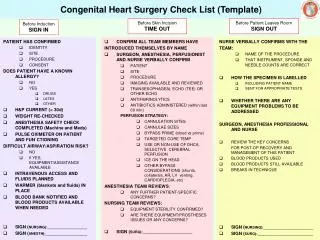
Implementation of a Surgical Safety Checklist for Congenital Cardiac Surgery(Intermediate Module)July 21, 2010
Schedule • April 21, 2010- Beginning Module • Introduction to checklist • July 21, 2010- Intermediate Module • Strategies for implementing the checklist • October 20, 2010- Advanced Module • Review of strategies to ensure sustained use following successful implementation
Agenda and Goals • What we have learned from our teleconferences with participating sites • Review checklist video as an example of how it may be used to improve safety • Review a strategy to successfully implement a checklist at your own institution • Next steps leading to the final webinar
What Have We Learned from Our Teleconferences? • Variable checklist utilization currently exists across sites • All sites have reported a high level of acceptance among operating room staff for adopting the checklist as an important safety intervention • Participation and leadership across sites for checklist implementation has been diverse and truly multidisciplinary!
What Have We Learned from our Teleconferences? • Most sites are still unsure how to move forward with recruiting additional local leaders • Most sites are still unsure how to implement a pilot phase to test the checklist • Most sites are still unsure how the checklist should be used in practice • All sites have the dedication and leadership necessary to succeed!
Introduction to Checklist Video • Video designed to demonstrate how the checklist can be used to facilitate communication between team members • Checklist content may change depending upon the local needs and culture of each hospital • Each section of the checklist will be presented separately to allow for questions and discussion • Please take note how the use of the checklist during each section may have to be changed to fit the needs of your own environment
Sign In Discussion • Are there any questions regarding the sign-in portion of the checklist? • Do any of the sites currently practice a sign-in or similar procedure prior to anesthesia induction? • For sites that do not perform a sign-in, are there any obstacles that you anticipate in adopting such a practice?
Time Out Discussion • Are there any questions regarding the time out portion of the checklist? • Do any of the sites currently practice a time out or similar procedure prior to anesthesia induction? • For sites that do not perform a time out, are there any obstacles that you anticipate in adopting such a practice?
Sign Out Discussion • Are there any questions regarding the sign-out portion of the checklist? • Do any of the sites currently practice a sign-out or similar procedure? • For sites that do not perform a sign-out, are there any obstacles that you anticipate in adopting such a practice?
Handover • Are there any questions regarding the handover portion of the checklist? • Do any of the sites currently practice a handover or similar procedure? • For sites that do not perform a handover, are there any obstacles that you anticipate in adopting such a practice?
How to Implement the Checklist: Strategies for a Successful Pilot Phase • Identify (and recruit!) leaders from each discipline • Nursing, anesthesia, Critical Care, surgery, and perfusion • Review of the checklist by each leader for feedback on content • How should it be changed to meet the needs of their discipline?
How to Implement the Checklist: Strategies for a Successful Pilot Phase • Modification of checklist from multidisciplinary feedback as necessary prior to piloting • Trial the checklist for 5-10 cases by pilot team • Make further adjustments to the checklist as necessary after obtaining further input
How to Implement the Checklist: Strategies for a Successful Pilot Phase • Recruitment of additional team members to pilot an additional 10-20 cases • Obtain further feedback on checklist content • Make final modifications to the checklist in preparation for operating room-wide use • Consider making posters for operating rooms and Intensive Care Units once the final version of the checklist is developed
Next Steps • Monthly teleconferences to assess progress and provide guidance as necessary • Time-lines for the pilot strategy previously discussed will depend upon the needs of each hospital • Frequent email correspondence is encouraged between teleconferences • IQIC@childrens.harvard.edu
Next Steps • Use of discussion boards on IQIC database (beginning next week) • Consider site visits to provide in-person assistance as needed • Next webinar will focus on strategies for ensuring sustained use of the checklist as your institution
Acknowledgements Shawn Rangel, MD, FACS Surgeon, Department of General Surgery David Roberson, MD, FACS Surgeon, Department of Otolaryngology Francis Fynn-Thompson, MD Surgeon, Cardiovascular Surgery Michelle Lyden, MSN, NP, MPA Quality and Safety Research Manager Traci Wolbrink, MD Chief Fellow, Pediatric Critical Care Patricia Hickey, PhD, RN, MBA, FAAN VP, Cardiovascular/Critical Care Services Jeanne Ahern, BSN, MHA, RN, CCRN Nurse Manager, CICU Annette Saltamartini Imprescia, RN, CCRN Clinical Educator, CICU Beverly Small, RN, CCRN Nurse, CICU Annette Schure, MD Anesthesia, Perioperative & Pain Medicine Patricia Galvin, RN, MSN, CNOR Clinical Coordinator, Cardiovascular Surgery Ravi Thiagarajan, MD Attending, Cardiology Department Kathy Jenkins, MD, MPH VP, Patient Safety and Quality Ashley Racine, BA Data Coordinator, PPSQ
Acknowledgements Laura Clark, BS Training Coordinator,Simulator Program, Division of Critical Care Medicine Kathryn Franklin, BS Nurse, Cardiovascular Surgery Gavin Hayes, BS System Specialist, Simulator Program, Division of Critical Care Medicine Susan Jay, RN, BSN, CNOR Nurse, Operating Room Gregory Matte, CCP, LP Perfusion Clinical Coordinator, Cardiovascular Surgery Peter Weinstock, MD Director, Simulator Program, Division of Critical Care Medicine