Download
1 / 51
510 likes | 525 Views
Explore the latest agents such as monoclonal antibodies and protein inhibitors for managing Indolent B-Cell Non-Hodgkin Lymphomas. Learn about promising studies and comparison between different treatments.

E N D
New Agents in Management of Indolent B-Cell NHLs F B Hagemeister MD Department of Lymphoma/Myeloma M D Anderson Cancer Center Las Vegas, Nevada February 27, 2014
Monoclonal Antibodies • Rituximab • Ofatumumab • Obinutuzumab • Protein Inhibitors • BTK Inhibitors • PI3K Inhibitors • Others • Immunomodulatory Agents New Agents in Management of Indolent B-Cell NHLs
Phase III MR, 2 Schedules, for Untreated FL Following SA Rituximab x 4: SAKK 35/03 • Med PFS: (MR = 4 doses, vs 5 years, both q 2 mo): • For all 165 enrolled: A-3.4 yr vs B-5.3 (p=0.14) • Thought due to higher relapse rate before MR begun for those in Gp A for “unexplained reasons” • For only those in remission at 8 mo: A-7.1 yr vs B-2.9 (p=0.004) • Gr 3-4 infections (Pt): A-1 vs B-5 • No differences in OS or ORR • Conclusion: If in remission after SA Rituximab, MR prevents relapse if given longer vs shorter interval Taverna et al, ASH 2013, # 508 But best duration of MR is still unclear.
The PRIMA Trial: A 6 Year Update Salles et al. ASH 2013, # 509. • Med f/u 73 months (from randomization) • 6 year PFS results: • 60% with R vs 42% without R (p<0.0001) • Favorable features affecting PFS by MVA: • OS rates, transformation rates not different • Still No result on differences related to type of chemotherapy administered
MR vs Obs after R-Chemo for FL: PFS in the PRIMA Trial Progression-Free Survival 24 72 Months Salles et al. ASH 2013 # 509
Early Relapse Of R-CHOP for FL: Effect of Early Relapse on OS Result Early Relapse in Lymphocare Study: <2 yrs from diagnosis (21% of 588 pts) By MVA: ER Associated with High LDH, PS > 1, Marrow DZ, and B Sx. Casulo et al. ASH 2013 # 510
90Y-Ibritumomab for Advanced Stage FL in First Remission: The FIT trial * All patients Note: Only 10-15% had received induction rituximab. A second randomized trial was planned with induction R-CHOP . High-risk pts receive RIT vs SCT, low risk receive RIT vs Obs. All would receive maintenance rituximab. But trial abandoned Hagenbeek et. al. ASH 2007, Abstract # 693
90YIbritumomab Consolidation vs MR for Untreated FL in CR/PR After R-CHOP Conclusion: MR is better than 90YIbritumomab after R-CHOP Lopez-Guillermo, et al. ASH 2013 # 369
Monoclonal Antibodies • Rituximab • Ofatumumab • Obinutuzumab • Protein Inhibitors • BTK Inhibitors • PI3K Inhibitors • Others • Immunomodulatory Agents New Agents in Management of Indolent B-Cell NHLs
Novel Anti-CD20 MoAbs for Relapsed/Refractory Indolent Lymphomas Morschhauser. Ann Oncol. 2010; Morschhauser. JCO. 2009;27: 3346; Negrea. ASH. 2009 (abstr 3757); Hagenbeek. ASH. 2009 (abstr 935); Hagenbeek. Blood. 2008;111:5486; Salles. ASH. 2009 (abstr 1704).
Monoclonal Antibodies • Rituximab • Ofatumumab • Obinutuzumab • Protein Inhibitors • BTK Inhibitors • PI3K Inhibitors • Others • Immunomodulatory Agents New Agents in Management of Indolent B-Cell NHLs
Obinutuzumab vs Rituximab for Rel iNHL: The GAUSS Study • 175 pt with rel CD20 pos iNHL, 149 had FL • Eligibility: CR or PR to rituximab-based therapy with response lasting > 6 months • Features: Median 2 prior Txs, others balanced • Therapy: G 1000 mg q wk X 4 or R X4. 4-6 wks later, pt with CR,PR,SD could receive drug q 2 mo X 2 yrs • Infusion-related RXNs more common with GA-101 (72% vs 49%, any Gr) • By IR panel, OR for all: G-42% vs R-24%; for FL: G-43% vs R-28% Sehn et al. ASH 2011, abst 269.
Obinutuzumab plus FC or CHOP for Rel/Ref FL: Phase I GAUDI Study • Obinutuzumab (GA-101): glycosylated, Type II moab against CD20 • 56 pt, stratified by prior therapy • Two Ob regimens chosen based on phase I trial: 1600 mg d 1+8, cycle 1, then 800 mg d 1+8 vs 400/400 for max 8 (CHOP) or 6 (FC) cycles • Toxicity: Not increased with higher doses of Ob • Results: OR=96% (G-CHOP), 93% (G-FC) CR=39%(G-CHOP), 50% (G-FC) • Basis for new G-CHOP study vs R-CHOP for untreated FL Radford et al: ASH 2011, abst 270.
Novel Therapeutics for Cancer Mahadavan and Fisher. JCO 29: 1876, 1884, 2011.
Novel Therapeutics for NHLs Mahadavan and Fisher. JCO 29: 1876, 1884, 2011.
Monoclonal Antibodies • Rituximab • Ofatumumab • Obinutuzumab • Protein Inhibitors • BTK Inhibitors • PI3K Inhibitors • Others • Immunomodulatory Agents New Agents in Management of Indolent B-Cell NHLs
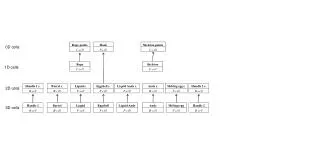
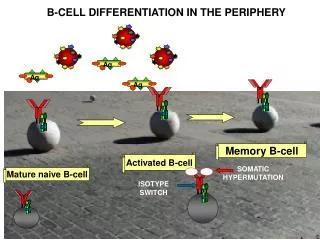
The B-Cell Receptor Pathway: A Useful Target in Therapy of B-Cell NHL • A transmembrane receptor protein on B cells • An antibody which binds antigen, inducing proliferation of plasma and memory B cells • Composed of two parts: • Ligand-binding moiety (IgM or IgD) • Signal transduction moiety (CD79) with an ITAM
Results of Activation of the B-Cell Receptor and Targets for Manipulation Idelalisib fostamatinib Ibrutinib ? enzastaurin ? temsirolimus everolimusdeferolimus bortezomibcarfilzomib
Phase I Ibrutinib for Relapsed NHL/CLL: Response Rates • * 1 CLL pt had nodal response, but increased lymphocytosis • **On the basis of decreased IgM Advani R, Fowler N et al. ICML 2011.
Phase I/II Trial of Ibrutinib for Ref/Ref MCL: Best Response by Patient Features Breakthrough approval for MCL and CLL granted by FDA 2013. Wang et al. NEJM 2013.
Ongoing studies: Placebo Controlled I + BR for Untreated MCL; I + R for Rituximab-Refractory FL
Monoclonal Antibodies • Rituximab • Ofatumumab • Obinutuzumab • Protein Inhibitors • BTK Inhibitors • PI3K Inhibitors • Others • Immunomodulatory Agents New Agents in Management of Indolent B-Cell NHLs
Idelalisib: Inhibitor of PI3K DeltaSelect Phase I Results in NHL (ASCO 2013) Fowler, N. ASH 2013 Education Session
Phase I Idelalisib for iNHL and MCL: Response Rates PFS Longer with Doses of 150 mg BID Kahl, B et al. ICML 2011.
Idelalisib Doses of 150 mg BID Were Associated With Longer PFS Results Kahl, B et al. ICML 2011.
Phase 2 Idelalisib for 125 Alkylator-Rituximab Ref iNHL: Nodal Response and PFS Results Maximum Nodal Response Median PFS = 11.4 months Historical Control: Bendamustine: DOR 10mo 53% ORR • 90% had improvement in lymphadenopathy • 57% had ≥50% decrease from baseline Gopal et al. ASH 2013 #85
Phase 1 Idelalisib for 40 Rel/Ref MCL: Dose 50-350 mg po BID Continuously ORR: 16 (40%), CR 3 (7.5%) ORR at < 150 = 29% (8/28), ORR with > 150 = 67% (8/12) Spurgeon et al. Lugano 2013.
Tumor Shrinkage in MCL Following Therapy with Idelalisib Kahl, B et al. ICML 2011.
Idelalisib + Bendamustine: Response Rates De Vose S, et al. ASH 2011 Abstract 2699.
Other PI3k Inhibitors for Rel/Ref FL: The ARD12130 Study and BAY 80-6046 • Phase II SAR245409: Inhibits Isos α, β, γ and δ, mTORC1, TORC2. • Study enrolls FL, CLL/SLL, MCL, and DLBCL. • Phase 2, Stage 1 results for FL (Gr 1, 2, 3A) reported. • Doses: 50 mg PO BID; Resp: ORR= 12/24 (50%), CR=2/24 (8%) • AEs: Diarrhea, Pneumonias, cataracts • BAY 80–6946, Inhibits Isoforms δ and α. May overcome resistance to PI3K-δ. • Phase II Study: 27 iNHL and 34 aggNHLs • Med Prior TXs: 3. Prior ASCT: 20% Brown et al. ASH 2013 # 86, Dreyling et al. ASH 2013 # 87.
Monoclonal Antibodies • Rituximab • Ofatumumab • Obinutuzumab • Protein Inhibitors • BTK Inhibitors • PI3K Inhibitors • Others • Immunomodulatory Agents New Agents in Management of Indolent B-Cell NHLs
Aurora Kinase A and B: Effects on the Cell Cycle Meraldi et al. Curr Op Genet Dev 2004.
Alisertib for Rel/Ref Aggressive NHLs: Response and Survival Rates • Response: ORR – 13/48 (27%), CR – 10% • Path: DLBCL-3/21, MCL-3/13, BL-1/1, Tr FL-2/5, TCL-4/8 Waterfall Plot Progression-Free Survival • Gr 3-4 Toxicities: Heme - ANC-63%, HGB-35%, PLT-33% Non-Heme – Stomatitis-15% Friedberg et al. JCO 32: 2014.
Alisertib in Aggressive B-Cell and T-Cell NHL: Response Rates • ORR: 32% (95% CI: 18-48) in overall population and responses observed in all histologic disease subtypes Friedberg J, et al. ASH 2011. Abstract 95.
Potential Effects of Anti-PD-1 Antibody in Therapy of Cancer Anti-PD-1 Antibodies: Pidilizumab, Nivolumab, Lambrolizumab McDermott and Atkins. Cancer Medicine 2: 662-673, 2013.
Phase 2 Anti-PD-1 (Pidilizumab) and Rituximab for Relapsed FL: Results • Response in 29 Evaluable Pts: OR-19 (66), CR-15 (52%) NO factor identified a poor response • Med Time to Response-88 days, with 6 more than 4 mo from initial infusion • Med PFS for all pts-18.9 mo • PFS Affected by FLIPI and FLIPI2 Scores PFS by FLIPI PFS by FLIPI2 Months Months Westin et al. Lancet Oncol 15: 69-77, 2014.
Phase 2 Anti-PD-1 (Pidilizumab) and Rituximab for Relapsed FL: Results Westin et al. Lancet Oncol 15: 69-77, 2014.
Monoclonal Antibodies • Rituximab • Ofatumumab • Obinutuzumab • Protein Inhibitors • BTK Inhibitors • PI3K Inhibitors • Others • Immunomodulatory Agents New Agents in Management of Indolent B-Cell NHLs
Cereblon A Target for Lenalidomide? Cereblon: Component of the E3 ubiquitin ligase complex Target protein for thalidomide, lenalidomide and pomalidomide These Inhibit the ubiquitin ligase activity May explain many of the known effects of immunomodulatory agents: Teratogenic activity Anti-myeloma activity T-cell activation
Tumor Cells IL-6 TNF IL-1 Tumor Stroma ICAM-1 Blood Vessels NFAT IL-2 IFN PKC IL-2 NK Cells VEGF bFGF CD28 PI3K CD8+ T Cells Dendritic Cells Lenalidomide: Targeting the Tumor Cell and Its Microenvironment Chng. Cancer Control.2005;12:91; Drach. Expert Rev Cancer. 2005;5:477.
Phase II Lenalidomide/Rituximab for Relapsed MCL: Response Duration Results for CR/PR patients (N = 24) Results for Patients with SD (N = 36) Goy et al. ASH 2012, abst 905.
Rituximab and Lenalidomide for Untreated iNHL: Study Design 7 8 9 10 11 12 1 2 3 4 5 6 Lenalidomide 20mg Days 1-21 Cycles 1-6* Lenalidomide 20mg Days 1-21 Cycles 7-12* Rituximab 375mg/M2 Day 1 of Cycles 1-6 Rituximab 375mg/M2 Day 1 of Cycles 7-12 R R R = RESTAGE If clinical benefit, can proceed to 12 cycles R R • Phase II, single institution • Planned Enrollment • 50 Follicular Lymphoma (grade I/II) • 30 Small Lymphocytic Lymphoma • 30 Marginal Zone Lymphoma • Groups analyzed independently for response and toxicity *For SLL patients: Dose escalation of lenalidomide starting with cycle 1: (10mg, 15mg, 20mg) Fowler N, et al ASH 2012.
Follicular Lymphoma Response by Tumor Burden and Molecular Features Fowler et al. ASH 2012, abst 901.
Lenalidomide Plus Rituximab as Initial Therapy for iNHL: Response Rates • Responses for FL independent of GELF criteria or disease bulk • Molecular responses for FL increased with treatment duration *Major or minor breakpoints from bone marrow, peripheral blood samples. Fowler et al. ASH 2012. Abst 901.
Lenalidomide/Rituximab for iNHLs: PFS by Histology Follicular Lymphoma Marginal Zone N=46 36 mo PFS: 81% N=27 36 mo PFS: 89% SLL N=30 36 mo PFS: 66% Fowler et al. ASH 2012, abst 901.
Lenalidomide-R for FcγRIIIa-F iNHLs or MCLs Refractory To Rituximab • FCGR3A polymorphisms cause significant impact on ORR, CR rate, and TTP after SA rituximab (ORR 26% and 2-Yr PFS of only 14% if F allele present). • Study: R-Refractory (SA or chemo combo) and F • Schema: 2 mo Len/Dex (10 mg QD/8 mg QWk, Part 1), then Rituximab q Wk X 4 with Len/Dex (Part 2), then continue Len/Dex alone. • Pts: 17/18 tested had F/F alleles, one V/V. Cartron 2002, Weng 2003, Chong et al. ASH 2013, #250.
Lenalidomide-R for FcγRIIIa-F iNHLs or MCLs Refractory To Rituximab Med f/u of 52 months, Med PFS is 24.5 months, 2 Yr PFS = 50% compared to 14% for historical controls. Chong, ASH 2013 # 250
Phase II Lenalidomide-R-CHOP for Untreated High- Risk (GELF) FL • Patients: 80 with FL Gr 1, 2, 3a; Med age 57, High LDH-40%, FLIPI 3-5 in 63%, Mass > 10 cm-25% • Therapy: Induction of Standard R-CHOP, plus Len 25 mg QD days 1-14, X 6 cycles + 2 R doses • Maintenance: MR q 8 wks X 2 yrs • Supportive: Pegfilgrastim day 4, QASA 10 mg QD • Med F/U 12 mo: ORR – 94%, CR/CRu – 74% • Gr 4 Toxicity: ANC-64%, PLT-12.5% • Gr 3 neuropathy: 36%, Gr 1-3 rash (2 Gr 3) • Thrombosis in 5 (3 catheter related) Tilly et al. ASH 2013 # 248
Rituximab Plus Lenalidomide 20 mg daily for 21 days, off 7 days X 6, and if CR, reduce to 10 mg