Download
1 / 28
280 likes | 294 Views
Indications for Initiation of ARV Therapy in Children Age >1 Year. Choice of Initial ARV Therapy. Use ZDV monotherapy only for prophylaxis in indeterminate infant in first 6 weeks of life Use combination ARV therapy with at least 3 drugs Slows disease progression Improves survival

E N D
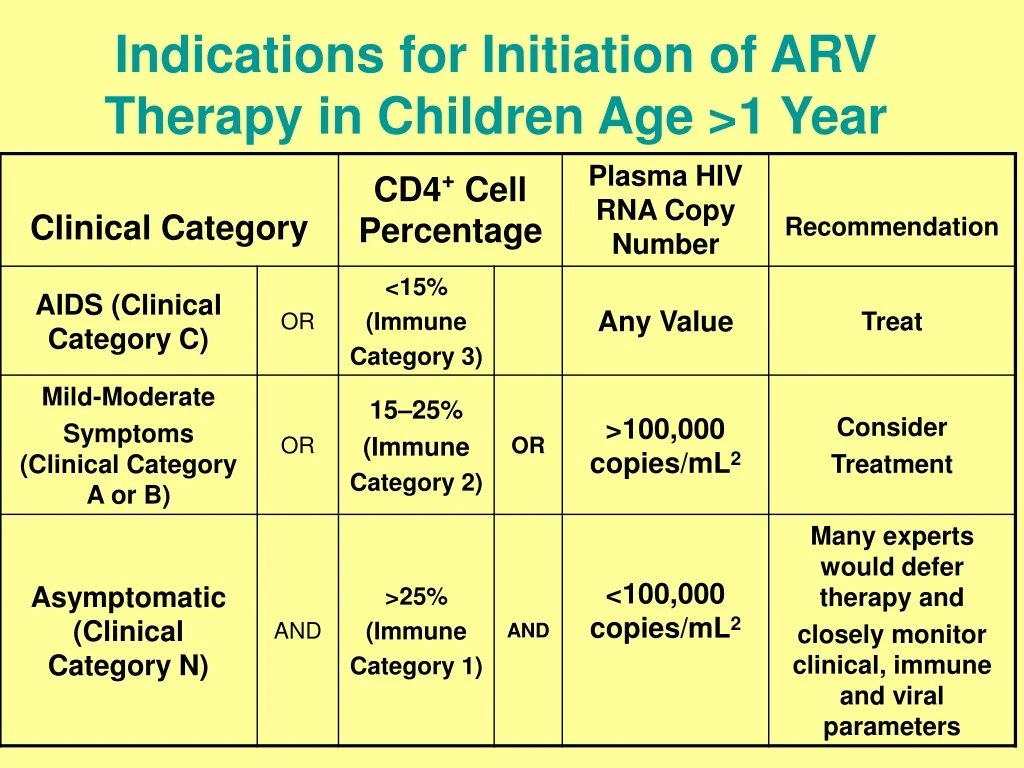
Indications for Initiation of ARV Therapy in Children Age >1 Year
Choice of Initial ARV Therapy • Use ZDV monotherapy only for prophylaxis in indeterminate infant in first 6 weeks of life • Use combination ARV therapy with at least 3 drugs • Slows disease progression • Improves survival • Sustains virologic response better • Delays development of resistance
Choice of Initial ARV Therapy • Maximal suppression of viral replication to undetectable levels, if possible, for as long as possible • Preservation or restoration of immune function • Prevention of complications of HIV infection, including opportunistic infections The goals of ARV therapy are:
Choice of Initial ARV Therapy • Consideration of resistance testing before initiation of therapy in newly diagnosed infants <12 months • Particularly if mother has known or suspecteddrug-resistant virus The Working Group recommends:
Recommendations on ARV Regimens for Initial Therapy • Data demonstrating durable viral suppression, immunologic and clinical improvement • Incidence and types of drug toxicity • Availability/palatability of formulations for children • Dosing frequency, food and fluid needs • Potential for drug interactions Working Group criteria:
Types of ARV Regimens for Children • PI-based (2 NRTIs + PI) • NNRTI-based (2 NRTIs + NNRTI) • NRTI-based (3 NRTIs)
Drug Regimen Categories for Initial Therapy • Strongly recommended • Recommended as an alternative • Offered in special circumstances • Not recommended • Insufficientdata for recommendation
Advantages Potent NNRTI-sparing Targets HIV at 2 steps Resistance requires multiple mutations Disadvantages High pill burden Multiple drug interactions Metabolic complications Poor palatability Few pediatric formulations PI-Based Regimens
Advantages Effective Palatable Less dyslipidemia/fat maldistribution PI-sparing Lower pill burden Disadvantages Cross resistance among NNRTIs Rare, but serious life-threatening skin rashes Hepatic toxicity Multiple drug interactions NNRTI-Based Regimens
Advantages Spares other classes of drugs Minimal drug-drug interactions Limited NRTI cross resistance Palatable Lower pill burden Disadvantages May be less potent than other regimens Rare, but serious lactic acidosis/hepatic steatosis Potential for ABC hypersensitivity NRTI-Based Regimens
Initial ARV Therapy: Not Recommended • Monotherapy—except ZDV prophylaxis for HIV exposed infants during the first 6 weeks of life • Certain 2 NRTI combinations • Antagonistic: ZDV/d4T • Overlapping toxicities: d4T/ddC, ddI/ddC, 3TC/ddC • Similiar structure and identical resistance: 3TC/FTC • Saquinavir: requires RTV boosting to achieve adequate drug level; pediatric dose unknown
Initial ARV Therapy: Insufficient Data to Recommend • Two NRTIs +delavirdine • Dual PIs (except lopinavir/ritonavir) • NRTI + NNRTI + PI (except EFV + NFV + 1 or 2 NRTIs) • Regimens containing • Emtricitabine (FTC) • Tenofovir • Atazanavir • Fosamprenavir • Tipranavir/ritonavir • Enfuvirtide (T-20)
Changing ARV Therapy • Failure based on virologic, immunologic, or clinical parameters • Toxicity or intolerance on the current therapy • Consider change if there is new data demonstrating that another regimen is superior to the current regimen AETC NRC
Virologic Considerations for Changing ARV Therapy • Less than 1.0 log10 decrease in HIV RNA from baseline 8-12 weeks after start of ARV therapy • HIV RNA not suppressed to undetectable levels after 4-6 months • Repeated detection in HIV RNA levels after undetectable levels on ARVs • A reproducible increase in HIV RNA after substantial response
Monitoring Virologic Response to Therapy Change • Assess virologic response within 4 weeks after initiating or changing therapy • Measure HIV RNA levels at least every 3 months • Resistance testing is recommended for persistent or increasing HIV RNA levels
Immunologic Considerations for Changing ARV Therapy • Change in immune classification • For children with <15% CD4+, persistent decline of ≥5% • Rapid and substantive decrease in CD4+ count (ie, >30% decline in <6 months)
Clinical Considerations for Changing ARV Therapy • Progressive neurodevelopmental deterioration • Growth failure despite adequate nutritional support • Disease progression
Changing ARVs for Toxicity/Intolerance • Choose drugs from same class with different toxicity/side effect profiles • Change of a single drug is permissible if a single drug can be identified as a cause of toxicity • Do not reduce dose below lower end of therapeutic dose range for the particular drug
Changing ARVs for Treatment Failure/Disease Progression • Assess and review adherence • Review patient medications • Perform resistance testing • Consider overlap in resistance • Change ARVs to contain at least 2 or 3 new ARVs • Consider clinical trials of investigational ARVs • Discuss quality of life issues
Adherence is Critical • ARV most effective in initial therapy • Poor adherence may enhance drug resistance • Child and caregiver participation is crucial • Assess, discuss and address adherence issues before initiating therapy
Adherence Issues in Children • Availability of drugs in palatable, liquid or mixable formulations • Difficulty of giving drugs that have food restrictions, because of children’s (particularly infant) eating schedules • Children’s dependence on caregivers for administration
Adherence Issues in Children • Timing issues, e.g., during school hours • Families’ reluctance to disclose HIV diagnosis may limit medication administration at daycare/school • Children’s developmental level influences ability and willingness totake medications
Denial and fear of their HIV infection Misinformation Distrust of the medical establishment Fear of ARV Lack of belief in the effectiveness of ARV Low self-esteem Unstructured and chaotic lifestyle Lack of familial and social support Adherence Issues in Adolescents
Adherence Issues in Adolescents • Adolescents’ readiness • Reminder systems, beepers, timers • Stylish pill boxes
Conclusion • Clinical care and treatment changes • U.S. Pediatric Guidelines Working Group meets monthly and reviews clinical trials result • Published text posted on www.aidsinfo.nih.gov • Current slide set with speaker notes posted on www.aidsetc.org
