Download
1 / 28
480 likes | 1.52k Views
Robertsonian chromosome translocations: the basics a tutorial to show how chromosomes which have been rearranged as a result of a Robertsonian translocation can segregate, and the clinical consequences. Professor P Farndon, Clinical Genetics Unit, Birmingham Women’s Hospital. 13.11.06.

E N D
Robertsonian chromosome translocations: the basics a tutorial to show how chromosomes which have been rearranged as a result of a Robertsonian translocation can segregate, and the clinical consequences Professor P Farndon, Clinical Genetics Unit, Birmingham Women’s Hospital 13.11.06
Chromosomal Translocations A translocation is formed when there has been transfer of material between chromosomes, requiring breakage of both chromosomes, with repair in an abnormal arrangement. If the exchange results in no loss or gain of DNA (ie genes), the individual is clinically normal and is said to have a balanced translocation. A balanced translocation carrier is, however, at risk of producing chromosomally unbalanced gametes. There are two types of translocation: reciprocal and Robertsonian (sometimes called centric fusion).
Reminder A reciprocal translocation usually involves breakage of two non-homologous chromosomes (ie one chromosome from each of two different pairs) with exchange of the fragments. Any of the pairs of chromosomes can be involved. The chromosome number remains at 46. The incidence of reciprocal translocations is about 1 in 500. There is a separate tutorial about these.
Reminder Areciprocal translocation usually involves breakage of two non-homologous chromosomes (ie one chromosome from each of two different pairs) with exchange of the fragments. Any of the pairs of chromosomes can be involved. The chromosome number remains at 46. The incidence of reciprocal translocations is about 1 in 500. There is a separate tutorial about these. Compare this reciprocal exchange with a Robertsonian translocation which involves only the acrocentric chromosomes (chromosomes 13,14,15 and 21, 22), and results in the formation of a “new” chromosome consisting of the whole of the long arms of the two acrocentrics involved, which have been fused together. The incidence of Robertsonian translocations in the general population is about 1 in 1000.
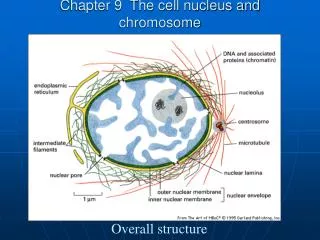
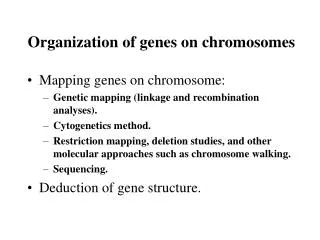
FZD2 AKAP10 ITGB4 KRTHA8 WD1 SOST MPP3 MLLT6 STAT3 BRCA1 GFAP NRXN4 NSF NGFR CACNB1 HOXB9 HTLVR ABCA5 Chromosome 17 CDC6 ITGB3 Reminder: chromosomes, genes and heredity • A chromosome is made of DNA (and histones) • Each chromosome contains its own set of genes in a linear order • There are two copies of each autosomal gene: one on each homologue
How do the unbalanced forms of a translocation cause clinical problems? • By altering the amounts of products of the genes involved • Three copies of genes (trisomic) • = 1.5 times normal amount • One copy of genes (monosomic) • = 0.5 times normal amount • Altered amounts may cause anomalies directly or may alter the balance of genes acting in a pathway
* named in honour of Dr WRB Robertson, an American who first described the fusion of two acrocentric chromosomes in his studies of insect speciation in 1916. Robertsonian* translocation Results from breakage of two acrocentric chromosomes (numbers 13, 14, 15, 21, 22) at or close to their centromeres, with subsequent fusion of their long arms to form one chromosome. An acrocentric chromosome has its centromere close to one end. The normal acrocentric chromosomes
The short arms of each chromosome are lost but this is of no clinical importance (as they contain genes for ribosomal RNA for which there are multiple copies on the other acrocentric chromosomes). The fact that the DNA structure on the short arms of the acrocentrics is so similar may be an important component in the formation of an individual family’s Robertsonian translocation. The total chromosome number is reduced to 45 as two of the acrocentrics have fused to form one (new) chromosome. Depending on where the breakage occurs, the resultant translocation chromosome can have one or two centromeres, but this has no functional effect.
As no gain or loss of important genetic material occurs, Robertsonian translocation carriers are normal. Once translocation chromosomes have been formed, they can be passed on to offspring. The commonest Robertsonian translocation is fusion between one chromosome 13 and one chromosome 14. A carrier for a Robertsonian (13;14) translocation Karyotype for a male carrier is descibed as: 45,XY,der(13;14)(q10;q10)
Although Robertsonian translocation carriers are asymptomatic, they can produce unbalanced gametes which can result in monosomic or trisomic zygotes. For instance, segregation of the chromosomes of a carrier of a Robertsonian 13;14 translocation can result in children with translocation trisomy 13 being born as shown here. Translocation trisomy 13 (Patau syndrome): three copies of chromosome 13 Although children with translocation Patau syndrome (trisomic for genes on chromosome 13) may be born alive, they usually die in the first few weeks or months of life. Trisomy 14 is lethal, as is trisomy for chromosomes 15 and 22 during early fetal life.
Although der(13;14)(q10;q10) is the most frequent Robertsonian translocation, the most important clinical effect of Robertsonian translocations arises from those involving chromosome 21 as they can result in the birth of children with translocation Down syndrome (trisomic for the genes on chromosome 21). In fact, second in frequency and clinically the most important Robertsonian translocation is der(14;21). Robertsonian translocations involving chromosome 22 are rare.
The clinical features of Down syndrome caused by either regular trisomy 21 or by a Robertsonian translcoation involving chromosome 21 are exactly the same because both result in three copies of the genes on chromosome 21. The recurrence risks for a family differ depending on whether the Down syndrome is caused by trisomy 21 or an unbalanced Robertsonian translocation.
The pedigree which follows shows the typical pedigree features associated with a Robertsonian translocation. What are they?
Died at birth: heart diseaseand blockage of bowel Age 42 Age 42 Down syndrome Age 20 Miscarriage at4 weeks Down syndrome
Mother young age (22 yrs) when child with Down syndrome born Children with features of Down syndrome in three generations Miscarriage early in pregnancy Died at birth: heart diseaseand blockage of bowel Age 42 Age 42 Down syndrome Age 20 Miscarriage at4 weeks Down syndrome
The affected people in this family havetranslocation Down syndrome. The Robertsonian translocation is between one chromosome 14 and one chromosome 21 This partial karyotype of the affected people shows an unbalanced karyotype:two copies ofchromosome 14 three copies ofchromosome 21
This is the partial karyotype of the father of the son with Down syndrome. It shows a balanced Robertsonian translocation: two copies of chromosome 14 and two copies of chromosome 21
How the three chromosomes of a Robertsonian translocation segregate at meiosis Usually two of them segregate together into one of the gametes at meiosis whilst the remaining chromosome segregates into another gamete. This means there are three possible ways in which the chromosomes will segregate, as described next.
Normal gamete The two “normal” chromosomes and the Robertsonian translocation chromosome in a carrier can segregate in three ways - segregation pattern 1 Fertilisation with a normal gamete
Normal gamete (Translocationtrisomy 14) The two “normal” chromosomes and the Robertsonian translocation chromosome in a carrier can segregate in three ways - segregation pattern 2 Fertilisation with a normal gamete
Normal gamete (Translocation Down syndrome) The two “normal” chromosomes and the Robertsonian translocation chromosome in a carrier can segregate in three ways - segregation pattern 3 Fertilisation with a normal gamete
(Translocation Down syndrome) (Translocationtrisomy 14) The two “normal” chromosomes and the Robertsonian translocation chromosome in a carrier can segregate in three ways - the 3 segregation patterns These three are lethal
As shown in the previous slide, of the possible segregants, monosomy 14, trisomy 14 and monosomy 21 are lethal. The remaining possibilities are • a child with normal chromosomes, • a child with the balanced translocation, and • a child with Down syndrome due to the unbalanced form of the translocation. A parent who is a carrier for a Robertsonian translocation involving chromosome 21 (as shown here) therefore has a high theoretical risk after conception of 1 in 3 of having a child affected with translocation Down syndrome.
But ... In clinical practice, the observed risk of having a liveborn child is less than this. For a female Robertsonian 14;21 carrier it is about 10%; for a male Robertsonian 14;21 carrier it is about 1%. This is thought to be due to loss through spontaneous miscarriage and perhaps effects of the translocation on meiosis or selection of sperm carrying the translocation. Compare these figures with the low recurrence in regular trisomy 21 Down syndrome (ie three structurally separate copies of chromosome 21). Regular trisomy 21 is due to an error in cell division, and has a recurrence risk of about 1 in 100. This is why it is important to karyotype a person with Down syndrome - to determine the chromosomal cause.
Most families with either reciprocal or Robertsonian translocations undertake fetal karyotyping (by chorionic villus sampling at about 10 weeks or amniocentesis at 16 weeks in pregnancy) to confirm that the baby has either the normal pattern of chromosomes, or the balanced form. An unbalanced karyotype is a recognised legal indication for ending a pregnancy.
How does a Robertsonian translocation occur in the first place? Most Robertsonian translocation carriers have inherited the balanced translocation chromosomes from a parent. Occasionally, however, the parents have normal karyotypes. The translocation in the offspring must have arisen de novo during the meiosis which produced the egg or sperm which formed the person with the translocation. About half the children with Down syndrome caused by an unbalanced Robertsonian translocation have the condition as a result of a de novo event.
Summary: Robertsonian translocation • Results from breakage of two acrocentric chromosomes (13, 14, 15, 21, 22) at or close to their centromeres, with subsequent fusion of their long arms to form one chromosome. • Individual clinically normal if no gain or loss of material (translocation carrier) • Unbalanced products may cause chromosomally abnormal baby, miscarriage, stillbirth, infertility • Other family members should be offered testing for carrier status
The end! • Thank you for completing this revision aid • We are interested in your comments about this aid. Please email Professor Farndon.(p.a.farndon@bham.ac.uk)