Download
1 / 14
140 likes | 298 Views
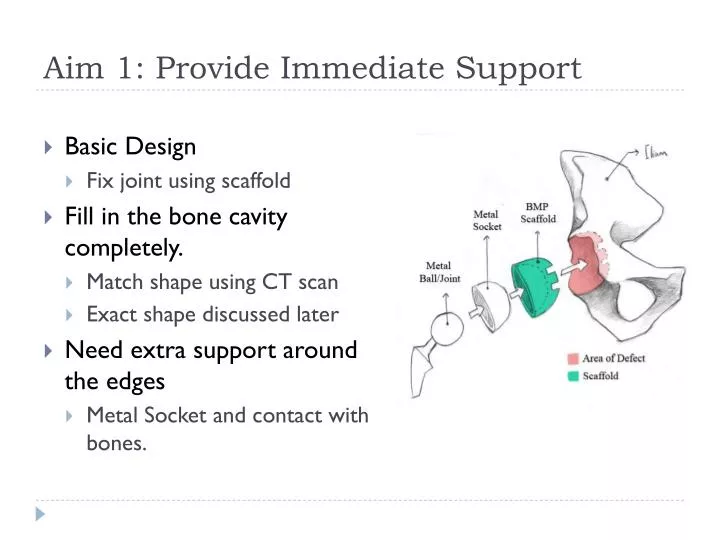
Aim 1: Provide Immediate Support. Basic Design Fix joint using scaffold Fill in the bone cavity completely. Match shape using CT scan Exact shape discussed later Need extra support around the edges Metal Socket and contact with bones. Aim 1: Provide Immediate Support.

E N D
Aim 1: Provide Immediate Support • Basic Design • Fix joint using scaffold • Fill in the bone cavity completely. • Match shape using CT scan • Exact shape discussed later • Need extra support around the edges • Metal Socket and contact with bones.
Aim 1: Provide Immediate Support • Extra support comes from BMP in scaffold • Most dense around the critical area • Fastest bone growth in critical area
Aim 1: limitations and failures • Forces on joint not always in one direction • For sake of discussion, think 2D first. • Force acting on center of the scaffold in the direction of the femoral neck is risky • May not always be safe for immediate walking for the patient
Aim 1: Alternative approach • Redistribute BMP gradient • Extra “pillar” in the affected region. • Supports the weight applied through the ball joint better.
Aim 2: provide improved bone growth • Design • BMP must cover all area by matching the patient’s bone shape • Use CT scan • Rapid prototype the scaffold. • BMP must avoid reconstructing bone too quickly • Osteoblasts and Osteoclasts • Rapid Prototyping • Cannot just “print” the scaffold • Using casting method
Aim 2: provide improved bone growth • As mentioned before… • BMP gradient • Most dense area used for immediate support • Least dense area used for slower but complete bone growth in inner region • Go slow to reduce risk!
Aim 2: Limitations and Failures • Limitation in using BMP • BMP may not be suitable for all patients • Case: patients with extra large amount of bone loss • Proportionally, these patients will lose more osteoblasts • Alternate approach • Attempt reducing amount of BMP used. • No change in gradient • Reduce overall usage of scaffold
Aim 2: Limitations and Failures 2 • Limitation in application • The scaffold match patient’s bone by shape, but how to match it physically? • There are some case where you cannot physically insert the scaffold
Aim 2: Alternate Approach 2 • “Simplify” the shape of the cavity using cement • Would require trimming of scaffold • Double CT scan may be necessary
Aim 2: Limitations and Failures 3 • Limitation in application • Can fail to insert it into patient if correct rotation is not recorded
Aim 2: Alternate Approach • Limitation in application • Not so bad. • Would need another device to correctly store the rotation in z-axis for the scaffold • Or make an “indicator” on the scaffold during rapid prototyping process.
Aim 3: Reduce Overall Number of Surgeries • 1. Successful bone growth would reduce risk of returning to the hospital • 2. Removing need to remove any of the component of scaffold reduce risk and need of returning to the hospital • Achieved this by making the scaffold using biodegradable material
Aim 3: Reduce Overall Number of Surgeries • Recall • Rate of bone growth = Rate which scaffold bio-degrades • Scaffold completely gone without causing excessive volume of BMP + scaffold in the joint for the patient • Limitations and Failures • Scaffold itself is not in gradient • At one point in time or space, amount of scaffold remaining may too little to hold BMP
Aim 3: Alternative Approach • Lower rate of bone growth • Reduce overall density of BMP in scaffold • It is safer if the scaffold remains a little bit longer than necessary