Download
1 / 65
650 likes | 849 Views
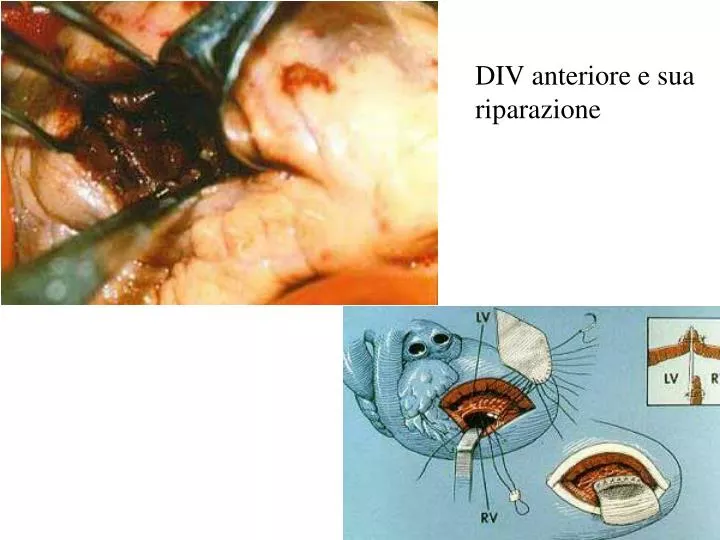
DIV anteriore e sua riparazione. Percutaneous transaortic closure of postinfarctional ventricular septal rupture. Hachida M, Nakano H, Hirai M, Shi CY. Department of Cardiovascular Surgery, Tokyo Womens' Medical College.

E N D
Percutaneous transaortic closure of postinfarctional ventricular septal rupture. Hachida M, Nakano H, Hirai M, Shi CY. Department of Cardiovascular Surgery, Tokyo Womens' Medical College. “We report a case of successful closure of a postinfarctional ventricular septal defect by means of the transaortic approach with a balloon catheter. This method brought about substantial improvement in cardiopulmonary function before an elective operation and made it possible to successfully perform the operation on the patient, an 81-year-old woman, on the 22nd day of admission”. PMID: 2012427 [PubMed - indexed for MEDLINE] Ann Thorac Surg 1991 Apr;51(4):655-7 Transcatheter closure of a residual postmyocardial infarction ventricular septal defect with the Amplatzer septal occluder D H Roberts,K P Walsh Blackpool Victoria Hospital, Whinney Heys Road, Blackpool, Lancashire FY3 8NR, UK, b Alder Hey Children's Hospital, Eaton Road, Liverpool L2 2AP, UKHeart 1998;80:522-524 ( November )
Rottura post-IMA di parete libera • William Harvey (1647). • Morgagni (1765) descrive 11 casi autoptici. (Ironicamente, Morgagni morì per questa complicanza!) • Hatcher e coll. (1970) all’Emory University riportano la prima riparazione chirurgica di rottura ventricolo destro • Fitz Gibbon e coll (1971) descrivono la prima riparazione chirurgica di rottura post IMA del ventricolo sinistro Rottura post IMA della parete anteriore Vsx. Decesso per tamponamento cardiaco acuto
Storia Naturale • Acuta: Morte improvvisa preceduta da crisi anginosa. Tamponamento e DEM (entro pochi minuti dall’esordio) • Subacuta: Breccia piccola temporaneamente chiusa da coagulo o adesione pericardica con lento filtraggio. Segni di tamponamento progressivo e poi shock cardiogeno. (D/d con estensione di IMA o IMA destro) Può essere compatibile con la vita per giorni. • Cronica: chiusura spontanea per adesione tra epicardio e pericardio o formazione di Pseudoaneurisma
Technique to repair rupture of the free wall of the left ventricle. A. Left ventricular free wall rupture. B. A limited infarctectomy is closed with horizontal mattress sutures buttressed with two strips of felt. C. Then the whole area is covered with a Teflon patch sutured to healthy epicardium with a continuous propylene suture. Alternatively, the Teflon patch can be glued to the ventricular tear and the infarcted area using a biocompatible glue. (Adapted from David TE: Surgery for postinfarction rupture of the free wall of the ventricle. In David TE [ed]: Mechanical Complications of Myocardial Infarction. Austin, TX, R.G. Landes Company, 1993, pp 142–151.)
Insufficienza Mitralica Post-IMA • Acuta (30-50% durante IMA) • Funzionale (“stunned heart”) Recupero • da rottura MP (0,5-1,5%) • MP Posteriore vs Anteriore: 3-6/1 • Malattia coronarica spesso Monovasale (25%) • Compare nella prima settimana • Cronica(10-15%) da disf. MP (reversibile “miocardio ibernato” od irreversibile) o da dilatazione Ventricolare (da dislocamento di MP). • Post IMA inferiore 3-5% • Post IMA anteriore 6-8% Malattia coronarica spesso Trivasale Compare fino a tre mesi post IM • Recidivante(2-5%) da “Claudicatio” di MP
Papillary muscle rupture and mitral valve insufficiency. This patient developed profound breathing problems (congestive heart failure) about one month before surgery. The congestive heart failure was a result of a ruptured mitral papillary muscle (caused by a heart attack), and fixed it by replacing the mitral valve. The papillary muscle and chordae typically knot themselves up in a very distinctive manner as seen here.
Insuff. Mitralica senza rottura di MP Infarction produces segmental dyskinesis of the papillary muscle base and some degree of ventricular dilatation at that level. Although the infarcted muscle may elongate acutely a small amount, healing by atrophy and fibrosis shortens the papillary muscle and displaces the base away from the mitral annulus to cause incomplete mitral valve closure.
Storia Naturale • Acuta • Rottura completa di MP: sopravvivenza media 3-4 gg • Rottura parziale di MP: sopravvivenza media 1-2 mesi • Cronica • 3 and 4+ • 1-year mortality of approximately 40 % • 2+ • 1-year mortality of approximately 17 % • 1+ • 1-year mortality of approximately 10 % • Overall 3/4+ IMR has a 30-day mortality of 24% and a 1-year mortality of 52%. • The onset of cardiogenic shock reduces survival to a few days.
Terapia • PTCA • Entro le 6 h dall’IMA • Trattamento di IM ischemica da disfunzione reversibile di MP • Chirurgica (associata a CABG): • Urgenza (shock non trattabile farmacologicamente) • Plastica Vavolare: (difficile da effettuare in acuto!) Mortalità 20% • SVM con conservazione, se possibile, dell’apparato sottovalvolare: riduce la mortalità dal 60% al 35%. • Elezione: Insufficienze mitraliche 3-4+ da alterazione anatomica dei MP (fibrosi o dislocazione per rimodellamento VS) • Plastica Valvolare (mortalità 15%) • Apparato Sottovalvolare (corde tendinee, muscoli papillari) • Lembi • Anulus • Sostituzione Valvolare con “chordal sparing techniques” (mortalità 30%)
Prognosi a distanza(at 5-year survival) • CABG + Plastica della Mitrale 91 ± 5 % • CABG + Sostituzione Valvolare Mitralica 43 ± 13 % Cohn LH, Rizzo RJ, Adams DH, et al: “The effect of pathophysiology on the surgical treatment of ischemic mitral regurgitation: Operative and late risks of repair versus replacement.” Eur J Cardiothorac Surg 1995; 9: 568.
Aneurisma del Ventricolo Sx • Aneurisma del Ventricolo sinistro:Area cicatriziale derivata dal muscolo dopo IM. Questa area è ben delimitata e presenta un’espansione sistolica (discinesi) • Pseudo-Aneurisma: dilatazione in connessione diretta con la cavità ventricolare, la cui parete deriva da coagulo organizzato. Esito cronico di una rottura di parete libera.
The aneurysm extended from the anterior descending coronary artery laterally, and from the atrioventricular groove, approximately 6 cm towards the apex of the ventricle
AnVs Trombizzazione di AnVs: causa di embolie arteriose sistemiche
Storia Naturale • Incidenza • 15-20% di IMA se non trattati • Incidenza ridotta con trombolisi: 7.6% (CASS Study) • Funzione Ventricolare • Globale rimodellamento e dilatazione ventricolare • Ridotta FE ( 35%) dovuta a movimento paradosso • Sopravvivenza (naturale) a 5 aa: 30-40% • Dimensione aumenta rischio di morte precoce • Se l’aneurisma è piccolo è legata ai fattori di rischio per CAD concomitanti • La prognosi è proporzionale alla funzione ventricolare • Cause di Morte: • aritmie (44%) • SC (33%) • IM ricorrente (11%) • Cause extracardiache (22%) • Rischio tromboembolico basso (0.35% paziente/anno)
Diagnosi Strumentale • ECG • RX • Ecocardiogramma • VCG
Coronal imaging of cine magnetic resonance imaging showing huge left ventricular apical aneurysm. LV = left ventricle AO = aorta AN = aneurysm.
Here, the apex of the heart has been opened, and scarred heart tissue is readily seen as whitish tissue (held by the clamps). Normal heart muscle (red) is visible inside the left ventricle, approximately 1-2 inches from the cut edge. A patch will be fashioned and anchored within the heart at the junction of the scarred and normal muscle.
A Dacron patch (ribbed, whitish material) has been tailored and sewn into the heart. The scarred tissue at the tip of the heart (held by clamps) will be sutured over the patch to complete the repair. This intracardiac baffle serves to septate the heart, and isolate the non-functioning portion of the left ventricle from the part that squeezes normally. This improves overall performance of the heart, and succeeded in relieving this patient's congestive heart failure, when medications alone had failed.
Complicanze post-operatorie: Mortalità operatoria: 5-10%
Pseudoaneurisma del Ventricolo sinistro • Può svilupparsi dopo una rottura acuta di un’area delimitata con emopericardio essere piccolo e contenuto che si organizza alla periferia e rimane in collegamento con la cavità ventricolare. • E’ caratterizzato da un colletto piccolo. • La parete è formata da pericardio adeso alla parete connettivale e si espande gradualmente. • Più spesso localizzato posteriormente che lateralmente. • Rottura più frequente che nell’aneurisma vero. • La diagnosi richiede l’intervento di resezione. Pseudo aneurisma apicale
Corso Integrato di medicina d’urgenza, terapia intensiva e infermieristica clinica applicata Lezioni di Cardiochirurgia Valvulopatie
Anatomy and Pathology 1. Crucial to understand the anatomy of the mitral valve in order or perform valve repair/surgery 2. Mitral valve is composed of five separate components: a. valvular leaflets b. annulus c. chordae tendinae d. papillary muscles e. left ventricular wall
Anatomy and Pathology 1. Crucial to understand the anatomy of the aortic valve in order or perform valve repair/surgery 2. Aortic valve is composed of five separate components: a. valvular cusps b. annulus c. Valsalva’s sinus d. sinus-tubular junction e. Aortic root
Positions of the aortic valve leaflets at end-diastole and end-systole and of a single leaflet in profile during ejection as the leaflet moves from the closed position (0) to full opening. Note how the fully opened leaflet tends to produce a unifom diameter above the ventricular-arterial junction to reduce turbulence that otherwise would be increased by the sinuses of Valsalva.
Pathology • Congenital Malformation • Rheumatic Disease • Degeneration • Endocarditis • Ischemic Valvulopaty
Rheumatic Aortic lesions • Fibrous thickening, • 3-cusp valve, • mild calcification, • rheumatic fever history in 50% aortic steno-insufficiency
Degeneration • Diffuse nodular calcification, • 3-cusp valve, • no commissural fusion Macroscopic appearance of healed, fibrous commissural fusion between left coronary cusp (right, held by forceps) and noncoronary (left) cusp of aortic valve
MS: Indications for Operation 1. asymptomatic patients are generally not recommended for operation 2. patients with severe mitral stenosis should undergo operation a. normal orifice is 4-6 cm2 b. 2-4 cm2 is mild c. 1-2cm2 is moderate d. < 1 cm2 is severe
MR: Indications for Operation • Acute symptomatic MR • Symptomatic or Asymptomatic Patients with LV Dysfunction: • TypeEFSystolic Dimension • Mild0.5-0.640-50 mm • Moderate0.3-0.550-55 mm • Severe<0.3>55 mm • (LV dysfunction will persist, symptoms diminish, risk increase) • Asymptomatic patients with atrial fibrillation or pulmonary hypertension (PAPm = >50 mmHg at rest, >60 mmHg exercise)
Surgical Options • Valve replacement • Mortality 2-7% • Anticoagulation • Decrease LV EF • Valve Repair (always preferable – feasible in 70-90% of pts) • Mortality 2-3% • No anticoagulation • Preservation of LV EF
The Perfect Valve • Excellent hemodynamics • Non-thrombogenic • Durable • Unrestricted availability • Easily implantable • Silent function • Low cost
Replacement Devices • Mechanical valves • Caged-ball • Monoleaflet • Bileaflet • Bioprostheses • Stented • Porcine • Pericardial • Stentless • Porcine • Bovine Pericardial • Homograft • Autograft
Braunwald Polyurethane mitral valve. First mitral valve replacement on March 11, 1960. Teflon chordae brought through the ventricular muscle and secured outside the heart Kay Mitral Valve.Teflon mitral valve prosthesis with artificial chordae.Implanted 1959 Original Starr-Edwards Mitral Valve. Lucite cage. Silastic rubber ball occluder. Implanted 1960. Harken double cage ball valve. Implanted in 1960
St Jude heart valve. The most popular bileaflet mechanical valve. First implant 1977. Pyrolytic carbon leaflets and housing. Tungsten impregna-ted leaflets. Modifications: low profile sewing cuff, and rotatable housing St Jude Quattro tissue valve. Investigational stentless quadracuspid tissue valve for mitral valve replacement. Bovine pericardium. Carpentier-Edwards Perimount Mitral valve. Bovine pericardial tissue valve with Eligloy stent."Stress-free" fixation. Lower profile mitral tissue prosthesis. Mitral Homograft
Flow characteristics • ball/cage < tilting dic < bileaflet • Thrombogenic potential • ball/cage > tilting disc > bileaflet • Aortic < Mitral < both
Anticoagulation Management (Machanical Prosthesis) • TIA is most common event • Standardization of coagulation management (INR) • Narrow therapeutic range: balance between thrombolic and bleeding risk • ACCP recommendations: INR 2.5-3.5 • Aortic: 2.5-3.0 • Mitral: 3.0-3.5 • Both: 3.5-4.0 • Appropriate use of antiplatelet therapy
Prevenzione delle infezioni su protesi La presenza di tessuto artificiale permette l’impianto di germi eventualmente presenti in circolo !!!!PROFILASSI ANTIBIOTICA!!!!
Mechanism of mitral insufficiency (Carpentier Classification) Type I (normal leaflet motion) Type II (leaflet prolapse) Posterior leaflet Anterior leaflet Both leaflets Type III (restricted leaflet motion)
Leaflet Prolapse (II): an excessive motion of a leaflet overriding the plane of the annulus in systole • Leaflet Restriction (III): an incomplete closure of a leaflet remaining beneath the plane of the annulus in systole