Download
1 / 1
20 likes | 160 Views
Introduction. Pattern 1: Mixed Hyper/Hypo-Metabolic Pattern. Conclusions/Discussion. Materials and Methods. Results. References. Before and After Therapy. Using PET to Diagnose NPALE. Pattern 2: Metabolic Pattern Mimicking Neurodegenerative Disease.

E N D
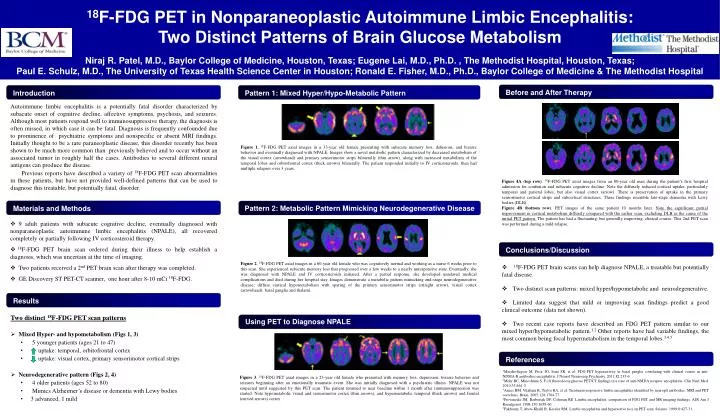
Introduction Pattern 1: Mixed Hyper/Hypo-Metabolic Pattern Conclusions/Discussion Materials and Methods Results References Before and After Therapy Using PET to Diagnose NPALE Pattern 2: Metabolic Pattern Mimicking Neurodegenerative Disease 18F-FDG PET in Nonparaneoplastic Autoimmune Limbic Encephalitis: Two Distinct Patterns of Brain Glucose Metabolism Niraj R. Patel, M.D., Baylor College of Medicine, Houston, Texas; Eugene Lai, M.D., Ph.D. , The Methodist Hospital, Houston, Texas; Paul E. Schulz, M.D., The University of Texas Health Science Center in Houston; Ronald E. Fisher, M.D., Ph.D., Baylor College of Medicine & The Methodist Hospital Autoimmune limbic encephalitis is a potentially fatal disorder characterized by subacute onset of cognitive decline, affective symptoms, psychosis, and seizures. Although most patients respond well to immunosuppressive therapy, the diagnosis is often missed, in which case it can be fatal. Diagnosis is frequently confounded due to prominence of psychiatric symptoms and nonspecific or absent MRI findings. Initially thought to be a rare paraneoplastic disease, this disorder recently has been shown to be much more common than previously believed and to occur without an associated tumor in roughly half the cases. Antibodies to several different neural antigens can produce the disease. Previous reports have described a variety of 18F-FDG PET scan abnormalities in these patients, but have not provided well-defined patterns that can be used to diagnose this treatable, but potentially fatal, disorder. Figure 1.18F-FDG PET axial images in a 33-year old female presenting with subacute memory loss, delusions, and bizarre behavior and eventually diagnosed with NPALE. Images show a novel metabolic pattern characterized by decreased metabolism of the visual cortex (arrowhead) and primary sensorimotor strips bilaterally (thin arrow), along with increased metabolism of the temporal lobes and orbitofrontal cortex (thick arrows) bilaterally. The patient responded initially to IV corticosteroids, then had multiple relapses over 3 years. Figure 4A (top row). 18F-FDG PET axial images from an 80-year old man during the patient’s first hospital admission for confusion and subacute cognitive decline. Note the diffusely reduced cortical uptake, particularly temporal and parietal lobes, but also visual cortex (arrow). There is preservation of uptake in the primary sensorimotor cortical strips and subcortical structures. These findings resemble late-stage dementia with Lewy bodies (DLB). Figure 4B (bottom row). PET images of the same patient 10 months later. Note the significant partial improvement in cortical metabolism diffusely compared with the earlier scan, excluding DLB as the cause of the initial PET pattern. The patient has had a fluctuating, but generally improving, clinical course. This 2nd PET scan was performed during a mild relapse. • 9 adult patients with subacute cognitive decline, eventually diagnosed with nonparaneoplastic autoimmune limbic encephalitis (NPALE), all recovered completely or partially following IV corticosteroid therapy. • 18F-FDG PET brain scan ordered during their illness to help establish a diagnosis, which was uncertain at the time of imaging. • Two patients received a 2nd PET brain scan after therapy was completed. • GE Discovery ST PET-CT scanner, one hour after 8-10 mCi 18F-FDG. Figure 2. 18F-FDG PET axial images in a 60-year old female who was cognitively normal and working as a nurse 6 weeks prior to this scan. She experienced subacute memory loss that progressed over a few weeks to a nearly unresponsive state. Eventually, she was diagnosed with NPALE and IV corticosteroids initiated. After a partial response, she developed unrelated medical complications and died during her hospital stay. Images demonstrate a metabolic pattern mimicking end-stage neurodegenerative disease: diffuse cortical hypometabolism with sparing of the primary sensorimotor strips (straight arrow), visual cortex (arrowhead), basal ganglia and thalami. • 18F-FDG PET brain scans can help diagnose NPALE, a treatable but potentially fatal disease. • Two distinct scan patterns: mixed hyper/hypometabolic and neurodegenerative. • Limited data suggest that mild or improving scan findings predict a good clinical outcome (data not shown). • Two recent case reports have described an FDG PET pattern similar to our mixed hyper/hypometabolic pattern.1,2 Other reports have had variable findings, the most common being focal hypermetabolism in the temporal lobes.3,4,5 • Two distinct 18F-FDG PET scan patterns • Mixed Hyper- and hypometabolism (Figs 1, 3) • 5 younger patients (ages 21 to 47) • uptake: temporal, orbitofrontal cortex • uptake: visual cortex, primary sensorimotor cortical strips • Neurodegenerative pattern (Figs 2, 4) • 4 older patients (ages 52 to 80) • Mimics Alzheimer’s disease or dementia with Lewy bodies • 3 advanced, 1 mild 1Maeder-Ingvar M, Prior JO, Irani SR, et al. FDG-PET hyperactivity in basal ganglia correlating with clinical course in anti-NDMA-R antibodies encephalitis. J Neurol Neurosurg Psychiatry. 2011;82:235-6. 2Mohr BC, Minoshima S. F-18 fluorodeoxyglucose PET/CT findings in a case of anti-NMDA receptor encephalitis. Clin Nucl Med. 2010;35:461-3. 3Ances BM, Vitaliani R, Taylor RA, et al. Treatment-responsive limbic encephalitis identified by neuropil antibodies: MRI and PET correlates. Brain. 2005;128:1764-77. 4Provenzale JM, Barboriak DP, Coleman RE. Limbic encephalitis: comparison of FDG PET and MR imaging findings. AJR Am J Roentgenol. 1998;170:1659-60. 5Fakhoury T, Abou-Khalil B, Kessler RM. Limbic encephalitis and hyperactive foci on PET scan. Seizure. 1999;8:427-31. Figure 3. 18F-FDG PET axial images in a 23-year old female who presented with memory loss, depression, bizarre behavior and seizures beginning after an emotionally traumatic event. She was initially diagnosed with a psychiatric illness. NPALE was not suspected until suggested by this PET scan. The patient returned to near baseline within 1 month after immunosuppression was started. Note hypometabolic visual and sensorimotor cortex (thin arrows), and hypermetabolic temporal (thick arrows) and frontal (curved arrows) cortex.






