Download
1 / 15
150 likes | 247 Views
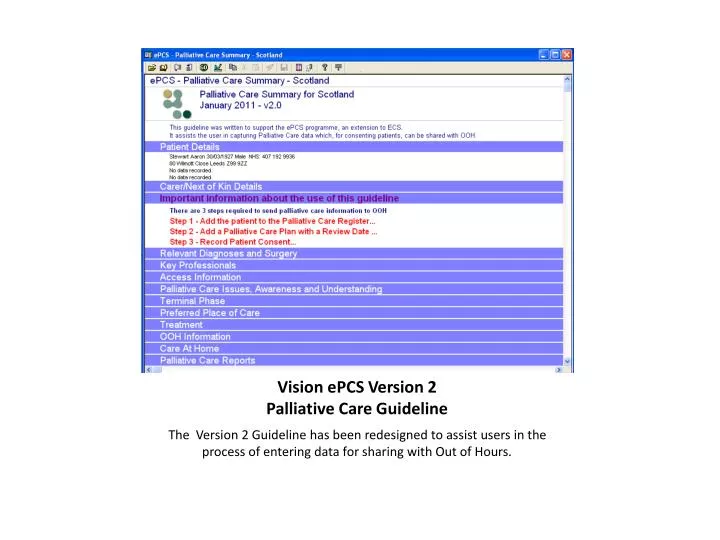
Vision ePCS Version 2 Palliative Care Guideline. The Version 2 Guideline has been redesigned to assist users in the process of entering data for sharing with Out of Hours. Step 1 – Palliative Care Register.

E N D
Vision ePCS Version 2 Palliative Care Guideline The Version 2 Guideline has been redesigned to assist users in the process of entering data for sharing with Out of Hours.
Step 1 – Palliative Care Register You can see whether the patient is already on the Palliative Care Register, if not, simply double-click to record one or more suitable terms from the list.
Step 2 – Palliative Care Plan The minimum data required to indicate the patient has a palliative care plan is the Review Date. You can also record whether the GP is willing to sign the death certificate in normal circumstances. This information can be updated at a later date if not yet known.
Step 3 – Patient Consent Palliative Care data can be entered as known, but the patient must have given consent to share Palliative Care data before it can be sent to OOH via the ECS extract. Record consent by selecting the Consultation menu, then Patient Registration. (See next slide...)
Step 3 – Patient Consent - Recording Doing it this way means the patient is already selected and all you need to do is click the Consent tab, then tick the box to record patient has given consent to share Palliative Care data. Click OK and return to entering data in Consultation Manager.
Relevant Diagnoses and Surgery From this section, you can choose which are the relevant diagnoses and/or surgical procedures to be notified to OOH. Highlight a record from the list, right click and choose the *GSFS1 option. Note: If you don’t see it on the list, click the button above marked “Add Palliative Care Problem” as described.
Key Professionals Here, you can record any other professionals involved in the care of the patient (if known). The latest record of each will be sent to OOH.
Access Information Use this section to record notes which might be useful in gaining access to the patient’s home in an Out of Hours situation. The type of notes should be set to Access Information (Hint – just hit the A key!)
OOH information – Additional Useful Information The Additional OOH Information section populates is equivalent to the “Special Note”. Only the most recent will be seen by the OOH staff and only 198 characters can be sent via ECS.
Patient and Carer Awareness and Understanding Here you can record any Palliative Care issues (up to 198 characters text) and also record what the patient’s and carer’s awareness and understanding of diagnosis and prognosis. Awareness is implicit in the Read code, however you may wish to use free text to convey patient and carer’s understanding of either diagnosis or prognosis.
Terminal Phase including DNACPR status In this section, you can access the Palliative Care plan to ensure Review Date and/or Death Certificate signing details are up to date. It is also particularly useful to let Out of Hours know the patient’s DNACPR status if known, or even to record that this is not known.
OOH Arrangements including Additional Useful Information for OOH This form can be used to inform OOH whether the GP wishes to be contacted Out of Hours and what has been discussed with the patient. The button marked Additional OOH Information button appears on the OOH Summary report in section 5h and is equivalent to the Special Note. Only the latest record is available to OOH staff.
Care at Home, includes ”just in case” drugs, catheter products, moving and handling equipment and syringe driver use Enter (or update) details relevant to this section. Note that OOH will only see the latest recorded entry and the first198 characters of free text.
The Palliative Care OOH Summary Report (Sections 1-2) Note that the Vision report includes full dosage information for repeat and acute medication, however the display of this will be truncated when it is extracted for ECS.