Download
1 / 28
290 likes | 316 Views
Learn about alcohol use, impacts, and related disorders in healthcare. Information on illicit drug use, diagnostic process, and developmental competence considerations. Recognize substance issues for better patient care.

E N D
Substance Use Assessment Chapter 6
Alcohol Use and Abuse • Alcohol • Most used and abused psychoactive drug • Given rates of alcohol use, it is not surprising that many patients in hospital and primary care find themselves with alcohol-related disorders • Morbidity and mortality data reflect adverse consequences of excessive alcohol use • Alcohol is involved in 40% of 41,000 annual deaths due to traffic accidents
Alcohol Use and Abuse(cont.) • Alcohol (cont.) • Emergency department visits attributable to alcohol from 1992 to 2000 was about 68.6 million, with an increasing trend of 18% • Alcohol consumption of four standard drinks per day or more associated with increased rates of death in men from: • Cirrhosis and alcoholism • Cancers of mouth, esophagus, pharynx, and liver combined • Injuries and other external causes
Alcohol Use and Abuse(cont.) • Alcohol (cont.) • In women, alcohol consumption increases risk of breast cancer in a dose-response relation, starting at an alcohol intake of about two drinks per day • Link between chronic alcohol use and liver disease is well known • Chronic heavy use increases risk of alcoholic cardiomyopathy, with an increase in left ventricular mass, dilation of ventricles, and wall thinning
Alcohol Use and Abuse(cont.) • Alcohol (cont.) • Hypertension is a common detrimental effect • Because of alcohol related morbidity, many patients encountered in primary care settings and in hospital will have significant drinking history • Alcohol dependence increases risk of sepsis, septic shock, and hospital mortality among intensive care unit (ICU) patients • Excessive alcohol use increases risk for ICU admissions due to trauma, hypothermia, and pancreatitis
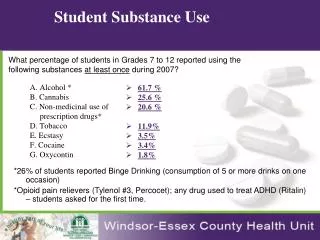
Defining Illicit Drug Use • About 8% of Americans aged 12 or older reported current illicit drug use in 2008 • Illicit drugs include marijuana/hashish, cocaine (including crack), heroin, hallucinogens, inhalants, or prescription-type drugs used nonmedically • Marijuana was most commonly used illicit drug with 6.1% of persons aged 12 or older reporting past month use
Defining Illicit Drug Use(cont.) • Illicit drug use has serious consequences for health, relationships, and for future jobs, school and career • Abuse of prescription drugs is fastest growing drug problem in U.S. • Three most frequently abused prescription opioid pain relievers were products using: • Oxycodone • Hydrocodone • Methadone
Diagnosing Substance Abuse • Rate of Americans classified with substance abuse or dependence • 9.2 % of the population aged 12 or older • 68% of those were dependent on or abused alcohol but not illicit drugs, and 14% used both alcohol and illicit drugs • Alcohol dependence or alcoholism is a chronic progressive disease that is not curable but is highly treatable • Accurate diagnosis needed for advice, intervention, appropriate treatment, and follow-up
Diagnosing Substance Abuse(cont.) • Gold standard of diagnosis is well defined in Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) • Alcohol problems under-diagnosed both in primary care settings and in hospitals • Excessive alcohol use often unrecognized until patients develop serious complications
Developmental Competence • Pregnant woman • Among pregnant women 15 to 44 • About 10.6% report current alcohol use • 4.5% reporting binge drinking and • 0.8% reporting heavy drinking • No amount of alcohol has been determined safe for pregnant women • Potential adverse consequences of alcohol use to fetus are well known • All women who are contemplating pregnancy or who are pregnant should be screened for alcohol use, and abstinence should be recommended
Developmental Competence(cont.) • Aging adult • Prevalence of current alcohol use decreases with increasing age • 67.4% among those 26 to 29 • 50.3% among those 60 to 64 • 39.7% among those 65 or older
Developmental Competence(cont.) • Aging adult (cont.) • Older adults have numerous characteristics that increase risk of alcohol use • Liver metabolism and kidney functioning decreases, increase availability of alcohol in blood for longer periods • Less tissue mass means increased alcohol concentration in blood • Older adults on multiple medications that can interact adversely with alcohol, including benzodiazepines, antidepressants, antihypertensives, and aspirin • Drinking alcohol increases risk of falls, depression, and gastrointestinal problems
Subjective Data • If patient is currently intoxicated or going through substance withdrawal, collecting any history data is difficult and unreliable • However, when sober, most people are willing and able to give reliable data, provided that setting is private, confidential, and nonconfrontational
Subjective Data(cont.) • Alcohol use • Ask about alcohol use • Do you sometimes drink beer, wine, or other alcoholic beverages? • If answer is “Yes,” then ask screening question about heavy drinking days, such as, “How many times in past year have you had five or more drinks a day (for men) or four or more drinks a day (for women)?”
Subjective Data(cont.) • Alcohol use (cont.) • To complete a picture of person’s drinking pattern, ask, “On average, how many days a week do you have an alcoholic drink?” and “On a typical drinking day, how many drinks do you have?” • Recommend person stay at moderate drinking patterns • Recommend even lower limits or abstinence for patients who take medications that interact with alcohol, who have a health condition exacerbated by alcohol, or who are pregnant (advise abstinence here)
Subjective Data(cont.) • Alcohol use (cont.) • Use brief screening instruments to help identify problem drinking and those who need more thorough assessment • AUDIT questionnaire • A quantitative form that has the advantage of letting the examiner document a number for a response so it is not open to individual interpretation • The AUDIT will help detect less severe alcohol problems (hazardous and harmful drinking) as well as alcohol abuse and dependence disorders
Subjective Data(cont.) • Alcohol use (cont.) • AUDIT questionnaire (cont.) • Helpful with emergency department (ED) and trauma patients because it is sensitive to current, as opposed to past alcohol problems • Useful in primary care with adolescents and older adults • Relatively free of gender and cultural bias • Note that AUDIT covers three domains • Alcohol consumption • Drinking behavior or dependence • Adverse consequences from alcohol • The AUDIT-C is shorter form helpful for acute and critical care units
Subjective Data(cont.) • Alcohol use (cont.) • The CAGE questionnaire (Cutdown, Annoyed, Guilty, Eye opener) • Works well in primary care settings because it takes less than 1 minute to complete • The CAGE tests for lifetime alcohol abuse and/or dependence • Does not clarify past problem drinking from present • Less effective with women and minority groups
Subjective Data(cont.) • Alcohol use (cont.) • Assess for alcohol use disorders using standard clinical diagnostic criteria • Determine whether there is a maladaptive pattern of alcohol use causing clinically significant impairment or distress
Subjective Data(cont.) • Alcohol use (cont.) • Ask, “In past 12 months, has your drinking repeatedly caused or contributed to: • Risk of bodily harm: drinking and driving, operating machinery, swimming? • Relationship trouble: family or friends? • Role failure: interference with home, work, or school obligations? • Run-ins with law: arrests or other legal problems?” • Ask, “In the past 12 months, have you not been able to stick to drinking limits, or repeatedly gone over them?”
Subjective Data(cont.) • Alcohol use (cont.) • Ask, “In past 12 months, has your drinking repeatedly caused or contributed to: • Shown tolerance: needed to drink more to get same effect? • Shown signs of withdrawal: tremors, sweating, nausea, or insomnia when trying to quit or cut down? • Kept drinking despite problems: recurrent physical or psychological problems? • Spent a lot of time drinking or anticipating or recovering? • Spent less time on other matters or activities that had been important or pleasurable?”
Subjective Data(cont.) • Alcohol use (cont.) • Ask about use of illicit substances • “Do you sometimes take illicit drugs or street drugs, such as marijuana, cocaine, hallucinogens, narcotics?” • If yes, ask, “When was last time you used drugs, and how much did you take that time?”
Subjective Data(cont.) • Screening women for alcohol problems • The TWEAK questions help identify at-risk drinking in women, especially pregnant women • Tolerance: how many drinks can you hold? Or How many drinks does it take to make you feel high? • Worry: have close friends or relatives complained about your drinking? • Eye-opener: do you sometimes take a drink in morning when you first get up? • Amnesia: has a friend or family member told you about things you said but could not remember? • Kut down: do you sometimes feel need to cut down?
Subjective Data(cont.) • Screening aging adults • Use the SMAST-G questionnaire for older adults who report social or regular drinking of any amount of alcohol • Older adults have specific emotional responses and physical reactions to alcohol and the 10 questions with yes/no responses address these factors
Subjective Data(cont.) • Advise and assist, brief intervention • Consequences of substance abuse are so debilitating and destructive to patients and their families that a short statement of assistance and concern is given here • If your assessment has determined the patient to have at-risk drinking or illicit substance use, state your conclusion and recommendation clearly • “You are drinking more than is medically safe.” • Relate to the person’s concerns and medical findings, if present; “I strongly recommend that you cut down, or quit, and I’m willing to help.”
Subjective Data(cont.) • Advise and assist, brief intervention (cont.) • If you determine the person has an alcohol use disorder, state your conclusion and recommendation clearly • “I believe that you have an alcohol use disorder.” • “I strongly recommend that you quit drinking, and I’m willing to help.” • Relate to the person’s concerns and medical findings, if present
Objective Data • Clinical laboratory findings give objective evidence of problem drinking • These are less sensitive and specific than self-report questionnaires • Useful data to corroborate subjective data • Serum protein, gamma glutamyltransferase (GGT) is most commonly used biochemical marker of alcohol drinking • Occasional alcohol drinking will not raise this measure, but chronic heavy drinking will • Be aware that nonalcoholic liver disease also can increase GGT levels in the absence of alcohol
Objective Data(cont.) • Clinical laboratory findings give objective evidence of problem drinking (cont.) • From complete blood count, the mean corpuscular volume (MCV) is an index of red blood cell size • MCV is not sensitive enough to use as only biomarker • Can detect earlier drinking after long period of abstinence • Breath alcohol analysis detects any amount of alcohol in end of exhaled air following a deep inhalation until all ingested alcohol is metabolized • This measure can be correlated with blood alcohol concentration (BAC) and is basis for legal interpretation of drinking