Download
1 / 31
310 likes | 458 Views
B ringing R esidencies t o F lorida. George Smith MD Medical Director Escambia Community Clinics Inc. Pensacola FL. overview. Introduction The Florida AHEC Network Patient Centered Medical Home National Workforce Statistics Florida Workforce Trends Recommendations Acknowledgements.

E N D
Bringing Residencies to Florida George Smith MD Medical Director Escambia Community Clinics Inc. Pensacola FL.
overview • Introduction • The Florida AHEC Network • Patient Centered Medical Home • National Workforce Statistics • Florida Workforce Trends • Recommendations • Acknowledgements
Escambia Community Clinic • Non-profit in Pensacola, Florida • Originally sponsored and owned by Sacred Heart Health System and Baptist Health Care • Established in January 1991 • Opened in November 1992. • Relocated in June 1994 • Federally Qualified Community Health Center (FQHC) in September 2007
Mission Statement • The mission of ECC is to provide quality outpatient primary and acute health care services to citizens of Escambia County and surrounding area. Escambia Community Clinics has a special focus to provide access to care for the under insured, uninsured, indigent and the medically needy regardless of their ability to pay for services.
Services • Acute Care - Family Practice Services • Routine family medicine • Hypertension control • Diabetic control • Women’s Health • Full laboratory services and x-ray • School, sports and work physicals • Workers comp • Escambia Community Clinics • Accepts most major insurances • Provides "walk-in" patient care • Appointments available
The 4 Functions of a Primary Care Medical Home • First Contact Care: “the door the patient knocks on to initiate help.” • Comprehensive: offering preventive, acute, chronic health care needs • Longitudinal: provides sustained relationships with people • Home Base: the place “from which other accommodations –specialists and other caregivers—are arranged.”
AAFP Medical Home • www.vcall.com/replay • 2071134629
We Need Doctors • Escambia Community Clinics, Inc., a non-profit outpatient primary care/ambulatory care facility is expanding and seeks a BC/BE Family Practitioner to join the medical staff. An excellent opportunity for exceptional personal and professional lifestyle. Position offers competitive salary, paid malpractice, paid vacation, paid CME and additional benefits.
AHEC • Extending Academic Resources to Medically Underserved Communities
AHEC • The concept of service/learning is now extensively used by AHEC as a means to accomplish its educational objectives for health professions students while delivering services to underserved populations. An AHEC service/learning program is accomplished through the extension and outreach efforts of academic faculty and students to community-based health programs that provide care to underserved populations. • Student enrichment activities are designed to influence underrepresented and/or disadvantaged youth to embrace the concepts of community health, diversity, individual health promotion and the potential for pursuing health careers. • By having a presence in local communities, AHECs have been able to promote community health and serve as vehicles for matching the educational needs of health professions faculty and students with the health care needs of local communities. Through these academic-community partnerships, AHECs have been able to produce a significant number of needed health services and community health projects.
The North Carolina Model • Since 1974, AHEC has created 339 primary care residency positions • 220 were in family medicine • 67% of the family medicine graduates stayed in the state to practice! • Residents trained at AHEC are more likely to practice in an underserved or rural community!
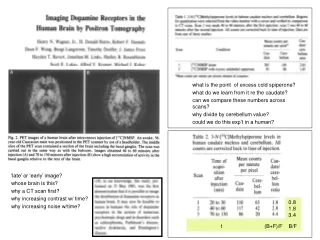
Primary Care Workforce Sept 2007 (1) • 97,752 family physicians/general practitioners (1 for every 3, 081 persons; 14.4% of the physician workforce). • 92,257 general internists (1 per 2,443 adults) and 48,930 general pediatricians (1 for 1,548 children and adolescents). • 238,939 primary care physicians (1 for every 1,260 persons).
COGME: Students and Residents • January 2005: Council of Graduate Medical Education: • A 15.0% expansion of allopathic medical student positions, • A 12.5% increase in residency positions over 10 yrs, • In 2006 AAMC increased the call to a 30% expansion • It is notable that the overall physician workforce grew at a rate twice that of the US population for the last decade and is projected to continue to outpace US population growth, without medical school expansion http://www.cogme.gov/report16.htm
Trends in Medical Schools • TREND 1: Decline of students from rural areas accepted into med school • 47% decline from 1976 – 2000 • Rural students applied at the same rate • Rural students are more likely to match in family medicine than urban students. • TREND 2: Residencies are seeing an increased number of US osteopathic students and students from non-US medical schools.
Minorities in Medicine • PREVIOUSLY: • Minorities were more likely to enter primary care and treat underserved populations • TREND: • Like their white peers, these groups are now choosing specialty careers over primary care
Internal Medicine Residents • Decreased interest in primary care • 50% drop from 1998 to 2003 • Increased desire to sub-specialize • 1998 54% chose primary care careers • 2003 27% made a similar choice
The Florida situation • Florida is one of the fastest growing states. • Population has increased 222 % from 1960 -2000 • Projected growth of 9.5 mil from 2000 -2030 • Population of elderly to grow by 124 %.Most likely to be in need of medical services • Largest increase in the elderly in Southeast Florida
The Florida Situation • Physicians practice where they attend residency • Nationally, Florida is ranked 46th for residency programs per 100,000 people in the state and 37th in number of med students • To meet the national ratio, Florida would need 2,700 more allopathic and osteopathic residency positions • Practically all Florida residency positions are filled.
If You Build It, They Will Come . . . • Nationally, 47% of residency graduates stay in state • In Florida, 60.5% stay in state • 2nd only to California Practice Path Followed by 2003 Community Hospital Education Program (CHEP) Completers *NOTE: 43 did not practice or continue training anywhere.
FSU COM • The Florida State University College of Medicine will educate and develop exemplary physicians who practice patient-centered health care, discover and advance knowledge, and are responsive to community needs, especially through service to elder, rural, minority, and underserved populations. • The curriculum is comprehensive, preparing students for any medical specialty and setting. Course content reflects the college’s mission, with special attention given to primary care, geriatrics, cultural diversity, and the needs of underserved populations. In addition, concentrated learning opportunities are offered for those students interested in rural health. All courses make use of the latest instructional technology, and medical informatics is integrated throughout the curriculum.
Rural Medical Education Track • The FSU College of Medicine recruits students into the "rural track" designed to send students to small rural communities for their third year and to encourage their return after graduation. Because of its strong medical community, Marianna, Florida was selected as the first rural community to begin this track.
“… Primary Care is the least expensive and most effective form of health care. It is key to addressing: • Disparities in health status and access to health care experienced by low income and/or underserved communities; • The epidemic of chronicdiseased, all preventable, in underserved communities; and • The requirement that any restructuring in the health care system be designed to address rising healthcare costs by preventing expensive and avoidable emergency room visits and hospitalizations….”
Recommendations • Invest in the development of a primary care workforce • Training and education programs need to be linked to primary care sites like CHC’s. • Medical school curriculum should be designed or revised to expose students to primary care and the primary care medical home model • Provide primary care role models to mentor and preceptor med students and residents.
Recommendations • Make primary care more attractive for med students by increasing reimbursement • Foster relationships between CHC’s and residency programs • Create new primary care residency programs using CHC’s as training sites.
Acknowledgements • Dr. David Nguyen • Sarah Cooke Third year med student FSU • Robert Graham Center • Laying the Foundation : The Primary care Imperative in New York Health reform