Download
1 / 33
370 likes | 733 Views
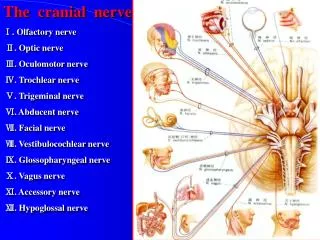
Therapy Considerations for the Radial Nerve. Sybil Hedrick, OTR/L, CHT, CSCS August 23, 2014 s ybil.hedrick@providence.org. Radial Nerve Innervation. Etiology.

E N D
Therapy Considerations for the Radial Nerve Sybil Hedrick, OTR/L, CHT, CSCS August 23, 2014 sybil.hedrick@providence.org
Etiology The regional anatomy of the nerve and its adjacent structures, as well as the nerve’s proximity to underlying bone and unyielding fascial bands, must be considered.
Muscle Loss:Axilla or Proximal Humerus • Weakness/paralysis of: • Tricep • Aconeous • Brachioradialis • All the muscles distal to brachioradialis
“Wrist Drop” Muscle Loss: Distal Humerus • Rests in a position of: • Forearm pronation • Wrist flexion • Thumb flexion & abduction • Slight MCP flexion • IP extension (some flexion if flexors are tight) • Unable to: • Extend wrist/fingers • Abduct/extend thumb
Muscle Loss:Forearm: Posterior Interosseous Nerve • Isolated involvement of the deep motor branch of the radial nerve • Present with strong radial deviation with extension of the wrist • Lack MP extension • Splinting is similar as for radial nerve palsy
Sensory Loss Sensory loss in Radial Nerve Palsy is not as much of a concern as compared to median/ulnar, address as applicable
Functional Loss • Cannot reach out with open hand to obtain objects • No stability at wrist for stable prehension • Difficult to write, type
Objectives Pre-Operative TherapyAnd/Or Conservative Management • Prevent deformity • Maintain tissue pliability • Promote neural regeneration and reorganization • Maintain function Radial Nerve Palsy often recovers spontaneously and will often not be rushed into tendon/nerve transfers so conservative management is key
Pre-Operative TherapyAnd/Or Conservative Management Evaluation • History • Sympathetic Function • Sensibility (tho not of a huge concern with radial nerve) • Motor Function • ROM: active and passive • Manual Muscle Testing • Be aware of substitution patterns • Dexterity
Splinting for Function • Goal to maximize current functional use of the hand/UE • Goal to harness wrist motion while allowing full finger flexion/extension • Try to recreate natural tenodesis motion to allow normal grasp/release of the hand * Note: a static wrist immobilization orthosis does not allow for functional grasp/release, covers palmar sensation and in the end, is not functional for the patient.
VanLede Radial Nerve Palsy Splint • Improved functional dexterity • Lower profile • Easier to get on/off for patient • Can use Delta Cast or Thermoplastic • Instructions for thermoplastic version can be found @ pattersonmedical.com search for Extension Assist Splint
Splinting to Prevent or Correct Deformity • Keep deneravated muscles from resting in an overstretched position • Prevent joint contractures • Enhance returning muscle function instead of allowing substitution patterns
Adaptations/Modifications • Cold intolerance frequently accompanies peripheral nerve injuries (PNI): neoprene mittens, gloves
Interventions: After Splinting • Modalities: • Heat • NMES • Nerve glides • Manual work • Home program • Repeated assessment to assist tracking of nerve recovery • Strengthening • Gravity eliminated • Aquatic therapy • Progressive resistance (PRE)
Preparationfor Tendon Transfer • Ideal, full if possible, PROM at joints which will be involved • Idea, full if possible, AROM as well • Proximal muscle strength should be at least 4/5 or better • The muscle to be transferred should have strength at least 4/5 or better
Motor Learning & Cortical Re-Mapping Motor Learning Cortical Re-Mapping • Motor Leaning aptitude should be assessed on the non-involved limb • Acquisition • Retention (consistency) • Transfer (flexibility) • Efficiency
Post-Operative TherapyRadial Nerve Tendon Transfer • Psychosocial Issues: client roles, motivation and compliance, cognition, past and current abilities/interests • Diminished success from transfer surgery can result with: • Denial • Frustration • Lack of trust in therapy program • Finances • Time • Must work closely with patient and Physician to eliminate and/or minimize or ease these factors
Post-Operative TherapyRadial Nerve Tendon Transfers • Pronator Teres to the ECRB for wrist extension • Palmaris Longus to rerouted EPL for thumb extension (if no PL, FDS (IV)) • FCR to EDC for finger extension (sometimes FCU is used) emedicine.medscape.com
Tendon Transfer Precautions • Common complications from tendon transfer include: • Excessive radial deviation at the wrist • Bowstringing of transferred tendons (EPL in particular) • Incomplete extension of 1 or more fingers • Incomplete finger flexion with simultaneous wrist flexion • Complete Rupture • Tendon adhesion • Therapist can play a key role in preventing some of these issues: • Careful monitoring of active motion, retrain movement patterns • Gradual progression out of splint • Ensure tendon gliding • Education, education, education every visit on stage of healing, phase of rehab
Post-Operative TherapyRadial Nerve Tendon Transfers • Splint picture • Splint out of surgery: ultimately depends on your surgeon! Sources vary between surgical and therapy resources. Usually 2-3 weeks • Elbow included, held in a position of pronation • wrist 30-50 deg of extension and 10-15 deg of UD • MCP’s at 0deg or 0-15 deg of flexion, finger IP’s free • Thumb fully abducted with IP in full extension
Motor Re-Education • Start with both the original motion combined with new motion • Start in gravity eliminated position and/or place and hold • Some resources say to use the opposite limb, however the wiring is now different?? • Slow, short session at a non-extreme force • Tips for specifics: • Wrist extension • Resist pronation to help facilitate wrist ext • Finger extension • Resist wrist flexion to help facilitate finger ext • Caution to NOT flex forcefully past neutral as this can stress the repair site • Thumb abduction/extension
Ther Ex Pearls Hammer Dynaflex
Post-Operative TherapyNerve Transfer for Radial Nerve Paralysis • Pre-operatively: Therapist should work on motor retraining using contralateral arm and normal movement patterns • Radial Nerve specific? Typing, reaching and grasping, playing instrument, etc. Tasks for wrist/finger extension, thumb abd/ex
Post-Operative TherapyNerve Transfer for Radial Nerve Paralysis • Post-operative pain management • Edema control • Immobilization • 7-10 days • Early ROM • Shoulder, trunk • 3-4 weeks: elbow, forearm, wrist and hand
MotorRe-Education • Must learn to coordinate new pathways for target muscle activation • Cortical command is now different and new • 1st: wrist/finger extension and thumb abduction muscle “contraction” combined with contraction from donor nerve: • FDS, FCR, PL • Want most synergistic action based on original motor pattern • Bimanual tasks • Motor reeducation with tasks that are normal for elbow flexion are instituted to relearn: • normal movement patterns • muscle recruitment • reestablish muscle balance
Strengthening • Utilize reinnervated muscle physiology and biomechanics • 1) short duration exercise sessions (<5-10min) • Slow onset contractions • begin in mid-range (place and hold) or gravity eliminated • 2) Multi-angle isometrics • 3) Concentric strengthening • 4) Eccentric strengthening