Download

1 / 63
630 likes | 775 Views
The Pediatric Heart. Congenital Heart Disease. CHD is a type of defect or malformation in one or more structures of the heart or blood vessels that occur before birth CHD affects 8-10 out of every 1,000 children Approximately 500,000 adults in the U.S. have congenital heart disease.

E N D
Congenital Heart Disease • CHD is a type of defect or malformation in one or more structures of the heart or blood vessels that occur before birth • CHD affects 8-10 out of every 1,000 children • Approximately 500,000 adults in the U.S. have congenital heart disease
Congenital Heart Disease • Symptoms in Adults • Shortness of breath • Limited ability to exercise • Symptoms in Children • Can be detected prenatally • Usually detected by the presence of a heart murmur, but not all CHD has a murmur, and not all murmurs are pathological!!!
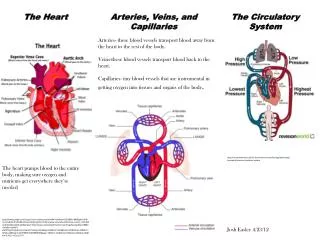
The Evaluation of the Heart • History • Physical Examination • Electrocardiogram • Chest radiograph • Echocardiogram and further evaluation by a cardiologist (cardiopulmonary stress test, 24- hour Holter monitor, ambulatory EKG, cardiac catherization, etc
The History • Ask about timing (at rest or activity-related), onset, and termination (gradual versus sudden), precipitating and relieving factors • Infants: • Cyanosis, squatting, loss of consciousness, tachypnea, diaphoresis, poor weight gain • Older children: • Dizziness, syncope, exercise intolerance, dyspnea on exertion, diaphoresis
The Physical Exam • Visual assessment of activity (agitation or lethargy) • Skin perfusion and skin color • Vitals: heart rate, respiratory rate, blood pressure (in all four extremities), and oxygen saturation • Dysmorphic features • Cardiovascular exam
Cardiac Defects in Syndromes • Down syndrome: AVSD • Turner syndrome: Bicupsid aortic valve, coarctation • Marfan syndrome: MVP, MR, dilated aortic root • Fetal alcohol syndrome: VSD, ASD • Maternal rubella: PDA, PPS
Cardiovascular Exam • Inspection & Palpation • Chest conformation (left precordial bulge from longstanding cardiomegaly) • Increased precordial activity • A diffuse point of maximal impulse • A precordial or suprasternal notch thrill • A palpable pulmonary (P2) at upper LSB
Cardiovascular Exam • Auscultation • The first heart sound (S1) is the sound of atrioventricular (AV) valve closure is best heard the lower left sternal border • The second heart sound (S2) is the sound of semilunar valve closure is best heard at the upper left sternal border. • S2 has a variable split (A2 and P2), that varies with respiration, non-variable can be cardiac disease
Cardiovascular Exam • Auscultation • The third heart sound (S3) is the sound of rapid filling of the left ventricle, it occurs in early diastole, after S2, and is medium- to low-pitched, usually only heard in the supine position. • The fourth heart sound (S4) is associated with atrial contraction and increased atrial pressure, its low-pitched, prior to S1 and usually not audible
Cardiovascular Exam • Auscultation • Ejection clicks are high-pitched, related to dilated great vessels or valve abnormalities • Occur anytime during systole: early, mid, or late • Early clicks at the mid LSB are from the pulmonic valve • Aortic clicks are best heard at the apex
Cardiovascular Exam • Auscultation • Murmurs should described by the following characteristics • Location and radiation • Relationship to cardiac cycle and duration • Intensity • Quality • Variation with position
Cardiovascular Exam • Location of pathology • RUSB • Aortic valve stenosis • LUSB • ASD • Pulmonary valve stenosis • LLSB • VSD inc AVSD • Apex • MR/MS/MVPS • Aortic stenosis
Cardiovascular Exam • Relationship to the cardiac cycle and duration • Systolic • Crescendo/decrescendo • Pansystolic • Throughout systole or the same intensity • Diastolic • Continuous • Systolic Ejection • ASD • Coarctation • Pansystolic • VSD • MR/TR • Diastolic • MS/TS • Continuous • PDS/AVM
Cardiovascular Exam • Intensity of murmur • Grade 1: soft, heard with difficulty • Grade 2: soft, but easily heard • Grade 3: loud without a thrill • Grade 4: loud with a precordial thrill • Grade 5: loud with a thrill heard with edge of stethoscope • Grade 6: loud with thrill and stethoscope off chest
Cardiovascular Exam • Quality of murmur: harsh, musical, or rough; high, medium, or low in pitch • Variation with position: audible when the patient is supine, sitting, standing, or squatting
Extracardiac Exam Arterial Pulse: Rate and Rhythm Quality and Amplitude of Pulse Arterial Blood Pressure Extremities Abdomen
Extracardiac Exam Rate and Rhythm Resting Heart Rates <1 month 80-160 1-3 months 80-200 2-24 months 70-120 2-10 years 60-90 11-18 years 40-90 • Rhythm should be regular, or with a phasic variation with respiration (sinus arrhythmia) is normal
Extracardiac Exam • Quality and Amplitude of Pulse • Pulses of upper and lower extremities should be equal • Bounding pulses are from run-off lesion, including PDA, aortic regurgitation, AVM, or any condition with low diastolic pressure (fever, anemia, or septic shock) • Narrow or thready pulses are from reduced cardiac output such as cardiomyopathy, myocarditis, pericardial tamponade, or severe aortic stenosis
Extracardiac Exam • Arterial blood pressure • Should be obtained in the upper and lower extremities • Systolic pressure in the lower extremities should be greater than or equal to that in the upper extremities • Extremities • Cyanosis, the mucous membranes • Clubbing • Edema, face and sacrum in the infant and young child
Extracardiac Exam • Abdomen • Hepatomegaly is the cardinal sign of right heart failure in the infant and child
Functional Murmurs • Murmurs are the most common reason for cardiology referral • Innocent or functional murmurs are common and 40-45% of children will have a functional murmur at some time during childhood
Functional Murmurs • Are always systolic murmurs, usually less than 3/6 • Often position-dependent, from supine to upright tend to disappear • Never associated with an ejection click or thrill • Are never evaluated when a child has a fever • The child is otherwise healthy and has a normal exam
Functional Murmurs • Newborn murmur • Peripheral arterial pulmonary stenosis • Still murmur • Pulmonary ejection murmur • Venous hum • Innominate or carotid bruit
Functional Murmurs • Location of functional or innocent murmurs • RUSB • Venous hum • LUSB • Pulmonary flow • Peripheral pulmonary stenosis • LLSB • Still murmur • Apex • Still murmur
Newborn Murmur • Heard in the first few days of life • Left lower sternal border, without significant radiation • Soft, short, vibratory grade 1-2/6 quality which subside with pressure to the abdomen • Disappears by age 2-3 weeks
PPS • Peripheral arterial pulmonary stenosis (PPS) • Heard with equal intensity at upper LSB, at the back, and in both axillae • Soft, short, high pitched, grade 1-2/6 systolic ejection murmur • Disappears by age 2
Still Murmur • Most common innocent murmur in young child • Heard between 2 and 7 years of age • Loudest between apex and LLSB • Musical or vibratory, short, high-pitched, grade 1-3 early systolic murmur • Loudest when patient is supine, diminishes or disappears with inspiration or when patient stands
Pulmonary Ejection Murmur • Most common innocent murmur in the older child • 3 years of age and older • Soft, systolic ejection murmur, grade 1-2/6 • Localized to the upper left sternal border • Louder when patient is supine
Venous Hum • Usually occurs after 2 years of age • Located in the infraclavicular areas and is usually louder on the right • Continuous musical hum of grade 1-2 intensity, maybe accentuated in diastole and with inspiration • Turning the child’s neck, placing the child supine, and compressing the jugular resolves the murmur
Innominate or Carotid Bruit • More common in older children and adolescents • Heard in the right supraclavicular area • Long systolic ejection murmur, harsh and of grade 2-3/6 intensity • Can be accentuated by light pressure on the carotid artery
Heart Sounds Normal Heart Sound Innocent Heart Murmur Split 2 Venous Hum VSD
Aquired Heart Disease • Kawasaki Disease • Rheumatic Heart Disease • Cardiomyopathy
Kawasaki Disease • First described in Japan in 1967 • Used to be called mucocutaneous lymph node syndrome • The etiology is unknown • No specific diagnostic test • Leading cause of acquired heart disease in children in the US
Kawasaki Disease • Median age at diagnosis is 2 years of age • 80% of patients are < 5 years of age • Male to female ratio is 1.5:1
Kawasaki Disease • Diagnostic criteria • Fever for more than 5 days and at least four of: • Bilateral painless, nonexudative conjunctivitis • Lip or oral cavity changes (eg, lip cracking and fissuring, strawberry tongue, and/or inflammation of the oral mucosa • Cervical lymphadenopathy (> 1.5 cm in diameter and usually unilateral • Polymorphous exanthem • Extremity changes (redness and swelling of hands and feet with subsequent desquamation)
Kawasaki Disease • Other non-diagnostic findings • GI • Vomiting diarrhea, gallbladder hydrops, elevated transaminases • Blood • Elevated ESR or CRP, leukocytosis, hypoalbuminemia, mild anemia in acute phase and thrombocytosis in subacute phase (usually second or third week of illness) • Renal • Sterile pyuria, proteinuria
Kawasaki Disease • Other non-diagnostic findings, cont. • Respiratory • Cough, rhinorrhea, infiltrate on chest radiograph • Joint • Arthralgia and arthritis • Neurologic • Mononuclear pleocytosis of cerebrospinal fluid, irritability, facial palsy
Kawasaki Disease • Cardiovascular complications • Myocarditis • Pericarditis • Valvular heart disease (usually mitral or aortic regurgitation) • Coronary arteritis (range from mild transient dilation to large aneurysm of coronary arteries)
Kawasaki Disease • Atypical Kawasaki • Patients with fever for at least 5 days, • But fewer than four of the diagnostic features, • And coronary abnormalities by echocardiography
Kawasaki Disease • Coronary artery lesions • Range from mild transient dilation to large aneurysms of coronary arteries • Aneurysms rarely occur before day 10 of illness • Untreated patients have a 15-25% risk of developing coronary aneurysms • Those at greatest risk are males, less than 6 months of age, and not treated with IVIG
Kawasaki Disease • Coronary artery lesions • Detected by two-dimensional echocardiography • Most resolve in 5 years • As aneurysms resolve, stenosis or obstruction can occur, up to 19 % • Giant aneurysms (>8mm) are less likely to resolve, and nearly 50% become stenotic • Acute thrombosis can occur, resulting in myocardial infarction, fatal in 20% of cases
Kawasaki Disease • Immediate management • Referral to Pediatric Emergency Department • IVIG and aspirin therapy • Echocardiogram’s immediately, at 2 weeks, and 6-8 weeks