Download
1 / 1
10 likes | 131 Views
The Skinny on Obesity in Texas: BMI in Texas Family Medicine Clinics. Kristin M. Yeung, Ramin Poursani, MD, Sandra K. Burge, PhD The University of Texas Health Science Center at San Antonio. Introduction. Methods.

E N D
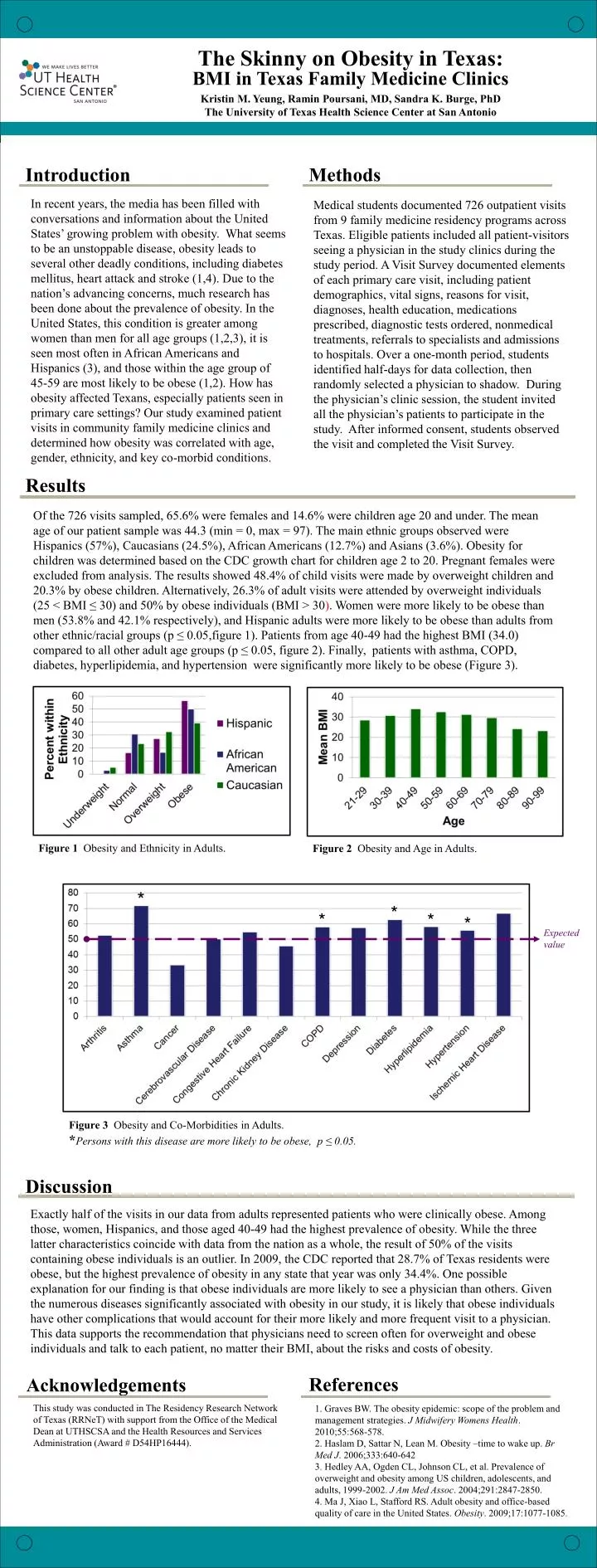
The Skinny on Obesity in Texas: BMI in Texas Family Medicine Clinics Kristin M. Yeung, Ramin Poursani, MD, Sandra K. Burge, PhD The University of Texas Health Science Center at San Antonio Introduction Methods In recent years, the media has been filled with conversations and information about the United States’ growing problem with obesity. What seems to be an unstoppable disease, obesity leads to several other deadly conditions, including diabetes mellitus, heart attack and stroke (1,4). Due to the nation’s advancing concerns, much research has been done about the prevalence of obesity. In the United States, this condition is greater among women than men for all age groups (1,2,3), it is seen most often in African Americans and Hispanics (3), and those within the age group of 45-59 are most likely to be obese (1,2). How has obesity affected Texans, especially patients seen in primary care settings? Our study examined patient visits in community family medicine clinics and determined how obesity was correlated with age, gender, ethnicity, and key co-morbid conditions. Medical students documented 726 outpatient visits from 9 family medicine residency programs across Texas. Eligible patients included all patient-visitors seeing a physician in the study clinics during the study period. A Visit Survey documented elements of each primary care visit, including patient demographics, vital signs, reasons for visit, diagnoses, health education, medications prescribed, diagnostic tests ordered, nonmedical treatments, referrals to specialists and admissions to hospitals. Over a one-month period, students identified half-days for data collection, then randomly selected a physician to shadow. During the physician’s clinic session, the student invited all the physician’s patients to participate in the study. After informed consent, students observed the visit and completed the Visit Survey. Results Of the 726 visits sampled, 65.6% were females and 14.6% were children age 20 and under. The mean age of our patient sample was 44.3 (min = 0, max = 97). The main ethnic groups observed were Hispanics (57%), Caucasians (24.5%), African Americans (12.7%) and Asians (3.6%). Obesity for children was determined based on the CDC growth chart for children age 2 to 20. Pregnant females were excluded from analysis. The results showed 48.4% of child visits were made by overweight children and 20.3% by obese children. Alternatively, 26.3% of adult visits were attended by overweight individuals (25 < BMI ≤ 30) and 50% by obese individuals (BMI > 30). Women were more likely to be obese than men (53.8% and 42.1% respectively), and Hispanic adults were more likely to be obese than adults from other ethnic/racial groups (p ≤ 0.05,figure 1). Patients from age 40-49 had the highest BMI (34.0) compared to all other adult age groups (p ≤ 0.05, figure 2). Finally, patients with asthma, COPD, diabetes, hyperlipidemia, and hypertension were significantly more likely to be obese (Figure 3). Figure 1 Obesity and Ethnicity in Adults. Figure 2 Obesity and Age in Adults. * * * * Expected value Figure 3 Obesity and Co-Morbidities in Adults. *Persons with this disease are more likely to be obese, p ≤ 0.05. Discussion Exactly half of the visits in our data from adults represented patients who were clinically obese. Among those, women, Hispanics, and those aged 40-49 had the highest prevalence of obesity. While the three latter characteristics coincide with data from the nation as a whole, the result of 50% of the visits containing obese individuals is an outlier. In 2009, the CDC reported that 28.7% of Texas residents were obese, but the highest prevalence of obesity in any state that year was only 34.4%. One possible explanation for our finding is that obese individuals are more likely to see a physician than others. Given the numerous diseases significantly associated with obesity in our study, it is likely that obese individuals have other complications that would account for their more likely and more frequent visit to a physician. This data supports the recommendation that physicians need to screen often for overweight and obese individuals and talk to each patient, no matter their BMI, about the risks and costs of obesity. References Acknowledgements This study was conducted in The Residency Research Network of Texas (RRNeT) with support from the Office of the Medical Dean at UTHSCSA and the Health Resources and Services Administration (Award # D54HP16444). 1. Graves BW. The obesity epidemic: scope of the problem and management strategies. J Midwifery Womens Health. 2010;55:568-578. 2. Haslam D, Sattar N, Lean M. Obesity –time to wake up. Br Med J. 2006;333:640-642 3. Hedley AA, Ogden CL, Johnson CL, et al. Prevalence of overweight and obesity among US children, adolescents, and adults, 1999-2002. J Am Med Assoc. 2004;291:2847-2850. 4. Ma J, Xiao L, Stafford RS. Adult obesity and office-based quality of care in the United States. Obesity. 2009;17:1077-1085.






