Download
1 / 20
200 likes | 321 Views
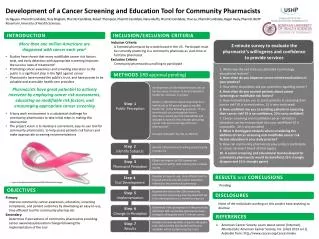
Top Ten Reasons Why Approval of Your IRB Application is Delayed. Richard Saitz, MD, MPH Chair, Institutional Review Board Boston University Medical Center. Top Ten Reasons for Delays. Insufficient information upon which to determine risk/benefit Benefit > Risk not made explicit

E N D
Top Ten Reasons Why Approval of Your IRB Application is Delayed Richard Saitz, MD, MPH Chair, Institutional Review Board Boston University Medical Center
Top Ten Reasons for Delays • Insufficient information upon which to determine risk/benefit • Benefit > Risk not made explicit • Study Design Inadequate • Informed consent Issues • Privacy/confidentiality Issues Not Addressed • Selection of Subjects Not Equitable or Described • Research and Clinical Care Difficult to Distinguish • Unethical Study • Administrative Details Not Addressed Appropriately • Response format
10. Response Format • Easily review-able response format facilitates and therefore speeds review • Delays may occur when response • Is that it was in the application • Does not include response to each administrative, protocol or consent issue • Not numbered, changes not highlighted
9. Administrative Details Not Addressed Appropriately • PI must be staff • Provide answers to all application questions • Names of persons with subject contact • Persons from other institutions and qualifications • Funding sources and amounts • Review by other IRBs • Visits for research purposes (beyond clinical care) • Prorate compensation • Coercion to participate • OSHA documentation
9. Administrative Details Not Addressed Appropriately • Lay summary • Signatures • Specific location of study • PI contact information • Employees, students as subjects
8. Unethical Study • Rare reason • Standard care withheld
7. Research and Clinical Care Difficult to Distinguish • Procedures already being performed for clinical purposes not used in research • Clinical versus research care not distinguished • Also a reason why ICF approval delayed • Specify that screening will occur after informed consent (unless part of routine care or minimal risk and consent not practical)
6. Selection of Subjects not Equitable or Described • Exclusion of uninsured • Targeting uninsured • Exclusion of non-English speakers • Benefits and burdens of research should be distributed fairly
5. Privacy and confidentiality Issues Not Addressed • Recruitment • Referral by the patient’s physician • Invitation by the patient’s physician • Self-referral • Publicly available information • Privacy during screening, consent • Anonymous versus confidential, justification • Be explicit about measures taken in protocol and ICF. • Certificate of Confidentiality
4. Informed Consent Issues • Reading level too high, language legalistic • Needs extensive revision (put yourself in subject’s shoes) • Risks of “simple,” “innocuous” tests not included (especially an issue for healthy normals) • Who is “your doctor?” • You are being asked to participate because… • Explain implications rather than simply stating risks (i.e. liver function test abnormalities)
3. Study Design Inadequate • Not clear • Not adequate, appropriate • Sample size not justified • Hypotheses to be tested not specified • Specify outcomes and comparisons • State what will be done with any data collected
3. Study Design Inadequate:“Pilot” or Exploratory/Descriptive • Justify design regarding what conclusions will be drawn (i.e. feasibility, adverse effects) • Inform subjects of purpose • Sample size may be justified by the need to assess variability in the sample or to look for large effects
2. Benefit > Risk not made explicit • Background not adequate • Benefits and risks attributed to, but not attributable to research • Nonsensical statements • Benefits: none • Risks: some • Conclusion: Benefits outweigh risks • Opinion stated but not explicitly supported
1. Insufficient Information Upon Which to Determine Risk/Benefit • Usual or standard care not clear • What is usual care here, elsewhere, the literature? • What are the benefits and risks of usual care or no care? • What is optimal care? • Benefits and risks (anticipated) not explicit • Quantify and compare • “Less anticipated” risks not identified (i.e. possibility that test or treatment could be worse than no test/treatment) • Absence of preliminary studies, justification for study
Do’s and Don’t’s • If not written down the Board doesn’t know it (IRB cannot make [best or worst case] assumptions) • All protocol issues need to be in the protocol (i.e. not just in the ICF) • Address regulations explicitly • Tell the IRB what is part of the research and what is not, explicitly • Don’t try to bypass the process (i.e. don’t send directly to Chair); materials will get lost, delayed • Specifically define inclusion and exclusion criteria
Do’s and Don’t’s • Be clear when a study is not testing a treatment, not testing treatment efficacy • Avoid cut and paste errors (very common) and checking off the wrong boxes • Be explicit when study will pay for care, and particularly regarding payment for screening procedures for ineligibles • Be explicit about differences between sponsor protocol/grant proposal and local study procedures • If research lab used, address any delays
Do’s and Don’t’s • Avoid typographical errors • Be explicit about why a drug study is exempt from an IND • Consistency throughout application • Avoid saying what has been approved in the past • Avoid asking for speedy review (whose protocol should be delayed)?
Do’s and Don’t’s • When pregnancy an exclusion, state how and when tested. In protocol (and consent) state risks to pregnant woman/fetus justifying exclusion. If there are genetic or fetal risks address partner risks • Don’t forget to address controls (when counting subjects, for recruitment, for ICF) • Ask substantive questions
IRB Guidebook Human Subject Protections - IRB Index Page • Foreword • Acknowledgments • Preface:* "How to Use the Guidebook" * • Introduction • Chapter I:Institutional Administration • Chapter II:Regulation and Policies • Chapter III:Basic IRB Review • Chapter IV:Considerations of Research Design • Chapter V:Biomedical and Behavioral Research: An Overview • Chapter VI:Special Classes of Subjects • Appendices • Glossary of Terms • Ordering Information: IRB Guidebook and Videotape • IRB Guidebook Prepared byRobin Levin Penslar, J.D.Research AssociateThe Poynter Center for the Study ofEthics and American InstitutionsOPRR Program OfficerJoan P. Porter, D.P.A.Office for Protection from Research Risks http://ohrp.osophs.dhhs.gov/irb/irb_guidebook.htm -- -- -- -- -- -- -- If you have questions about human subject research, click ohrp@osophs.dhhs.govIf you have questions/suggestions about this web page, click Updated