Download
1 / 24
240 likes | 343 Views
The Obesity Challenge: Levels, Consequences and Proposed Interventions in Ghanaian Women. Allan G. Hill Dept. of Social Statistics and Demography. The Broad Outlines of the Problem. At much lower income levels, obesity is equally common in many African urban populations

E N D
The Obesity Challenge: Levels, Consequences and Proposed Interventions in Ghanaian Women Allan G. Hill Dept. of Social Statistics and Demography
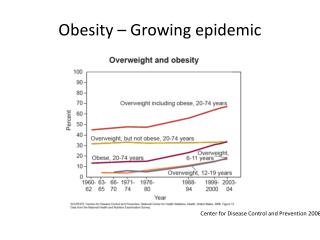
The Broad Outlines of the Problem • At much lower income levels, obesity is equally common in many African urban populations • The rates of obesity are higher everywhere for women • Adult obesity and childhood under-nutrition exists side by side • Dietary change and increased exercise regimens are more difficult in lower income societies
Obesity levels compared: BMI >30 in adults over age 16. Source: OECD Health Data 2012 - Version: October 2012
Correlates of obesity and overweight in Accra women 2010 Benkeser, Biritwum and Hill. 2012 Ghana Med J 46(2): 66-75.
Accra women: measured body heights and weights by age in 2010
Evidence on preferences: “current’’ body silhouette compared with “ideal” and “healthiest”.
Intervention options • Contextual interventions • School meals, physical education • Pricing and availability of fatty foods • Urban planning and transport arrangements • Community and social interventions • Fitness and sport promotion: clubs • Obesity as a preventable illness • Individual • Diet and exercise • Weight watchers and the like...
Small Steps. Big Rewards. A GAME PLAN to Prevent Type 2 Diabetes • Diabetes prevention and management c.f. Obesity directly • GAME PLAN • 50 small steps, not a single intervention (e.g. Weight Watchers) • Food and activity tracker • Fat and calorie counter
Scientific evidence The Diabetes Prevention Program (DPP) was a major clinical trial, or research study, aimed at discovering whether either diet and exercise or the oral diabetes drug metformin could prevent or delay the onset of type 2 diabetes in people with impaired glucose tolerance (IGT). The DPP found that over the three years of the study, diet and exercise sharply reduced the chances that a person with IGT would develop diabetes. Metformin also reduced risk, although less dramatically. The DPP resolved these questions so quickly that, on the advice of an external monitoring board, the program was halted a year early. New England J of Med February 7, 2002
10-year follow-up of diabetes incidence and weight loss in the Diabetes Prevention Program Outcomes Study • During the 10·0-year (IQR 9·0—10·5) follow-up since randomisation to DPP, the original lifestyle group lost, then partly regained weight. The modest weight loss with metformin was maintained. • Diabetes incidence rates during the DPP were 4·8 cases per 100 person-years (95% CI 4·1—5·7) in the intensive lifestyle intervention group, 7·8 (6·8—8·8) in the metformin group, and 11·0 (9·8—12·3) in the placebo group. • Diabetes incidence rates in this follow-up study were similar between treatment groups: 5·9 per 100 person-years (5·1—6·8) for lifestyle, 4·9 (4·2—5·7) for metformin, and 5·6 (4·8—6·5) for placebo. • Diabetes incidence in the 10 years since DPP randomisation was reduced by 34% (24—42) in the lifestyle group and 18% (7—28) in the metformin group compared with placebo. • The Lancet, Volume 374 (9702):1677 - 1686, 14 November 2009
Study design: Phase 1 • Since this is a community study and not clinic or hospital based, we shall select our participants from the population of 3200 women already enrolled in the WHSA and for whom we have prior health information. • This will make the identification of those most at risk simpler. • To select the at-risk women, we shall stratify the EAs by socio-economic status (variables taken from the 2000 census) in which the WHSA women live and identify 20 women in each of 6 contrasting communities defined as follows: • Ethnicity – language group • Socio-economic status of the neighbourhood
Community strategy • In each neighbourhood, identify the most active relevant civil society actors. • Some may be church or mosque based groups but the investigators have already worked with associations such as the Mothers and Baby Clubs, the Nima-Mamobi-Newtown Human Rights City initiative and have been supported by city councillors known as Assemblymen and Women who are elected to the Accra Metropolitan Area Council. • Focus groups to obtain general reactions to the ‘Power to Prevent’ approach and then after adaptation, translate the materials into the three main languages
Key qualitative research • More information about food groups, food intake, portion sizes and ingredients (already begun). • From exhaustive list of Small Steps, agree on the (less than 50!) that would form the menu offered to community groups of women. • Develop diaries with language accessible to women from different language groups
Enrollment and follow-up • Women enrolled and held in the program for 3 months. • Record which behaviours are most readily adopted and record blood pressure, weights, heart rate, and waist and hip measurements for all the participating women. • At the end of 3 months, new focus groups to gather the women’s reactions to the interventions. • The Ghana School of Public Health to convene a meeting of stakeholders (Ghana Health Services and the leading NGOs able to take on the program themselves) and make recommendations for next steps. • Basis for full-scale trial of the approach to a much larger set of at-risk women.
Examples of the 50 or so steps used in the US trials • Reduce Portion Sizes • Put less on your plate, Nate. • 1. Drink a large glass of water 10 minutes before your meal so you feel less hungry. • 2. Keep meat, chicken, turkey, and fish portions to about 3 ounces. • Eat a small meal, Lucille. • 4. Use teaspoons, salad forks, or child-size forks, spoons, and knives to help you take smaller bites and eat less. • 5. Make less food look like more by serving your meal on a salad or breakfast plate. • How much should I eat? • Try filling your plate like this: • 1/4 protein • 1/4 grains • 1/2 vegetables and fruit • dairy (low-fat or skim milk)
Move More Each DayFind ways to be more active each day. Try to be active for at least 30 minutes, 5 days a week. • Walking is a great way to get started and you can do it almost anywhere at any time. Bike riding, swimming, and dancing are also good ways to move more. • Dance it away, Faye. • 8. Show your kids the dances you used to do when you were their age. • Let's go, Flo. • 11. Deliver a message in person to a co-worker instead of sending an e-mail. • 12. Take the stairs to your office. Or take the stairs as far as you can, and then take the elevator the rest of the way.
Choose to eat more vegetables, fruits, and whole grains. Cut back on high-fat foods like whole milk, cheeses, and fried foods. This will help you reduce the amount of fat and calories you take in each day. • Snack on a veggie, Reggie. • 17. Buy a mix of vegetables when you go food shopping. • 18. Choose veggie toppings like spinach, broccoli, and peppers for your pizza. • Cook with care, Claire. • 22. Stir fry, broil, or bake with non-stick spray or low-salt broth. Cook with less oil and butter. • Cook in style, Kyle. • 25. Cook with a mix of spices instead of salt. • 26. Try different recipes for baking or broiling meat, chicken, and fish. • Eat healthy on the go, Jo. • 29. Have a big vegetable salad with low-calorie salad dressing when eating out. Share your main dish with a friend or have the other half wrapped to go.
Drinking and snacking • Rethink your drink, Linc. • 33. Find a water bottle you really like (from a church or club event, favourite sports team, etc.) and drink water from it every day. • Eat smart, Bart. • 37. Eat foods made from whole grains every day, such as whole wheat bread, brown rice, oats, and whole grain corn. • 42. Eat a healthy snack or meal before shopping for food. Do not shop on an empty stomach. • Keep track, Jack. • 44. Make a list of food you need to buy before you go to the store. • Read the label, Mabel. • 46. Compare food labels on packages.
Risks and expectations • Moving more in near-equatorial Africa is hot and uncomfortable... • The urban environment is polluted and pavements are rough and dangerous with little green open space except the beach • Portion control is difficult when cooking and eating is a collective activity • BUT social cohesion is strong and obesity is now part of the national debate
Signs of public engagement:Accra, March 22, 2014 GNA • Ghana has the largest number of overweight and obese people of over three million out of the estimated population of 20 million, statistics on the prevalence of overweight and obesity in seven African countries have shown. • The countries are Ghana, Congo Brazzaville, Liberia, Nigeria, Niger, Senegal and Sierra Leone. • Health Minister Major Courage Quashigah (Rtd) made this known in a speech read on his behalf at a health Symposium on the Prevalence of Obesity in Ghana in Accra on Thursday. • Overweight and obesity, which were considered problems only in high -income countries, were dramatically on the rise in low and middle-income countries particularly in urban settings, the minister noted.