Download
1 / 47
490 likes | 777 Views
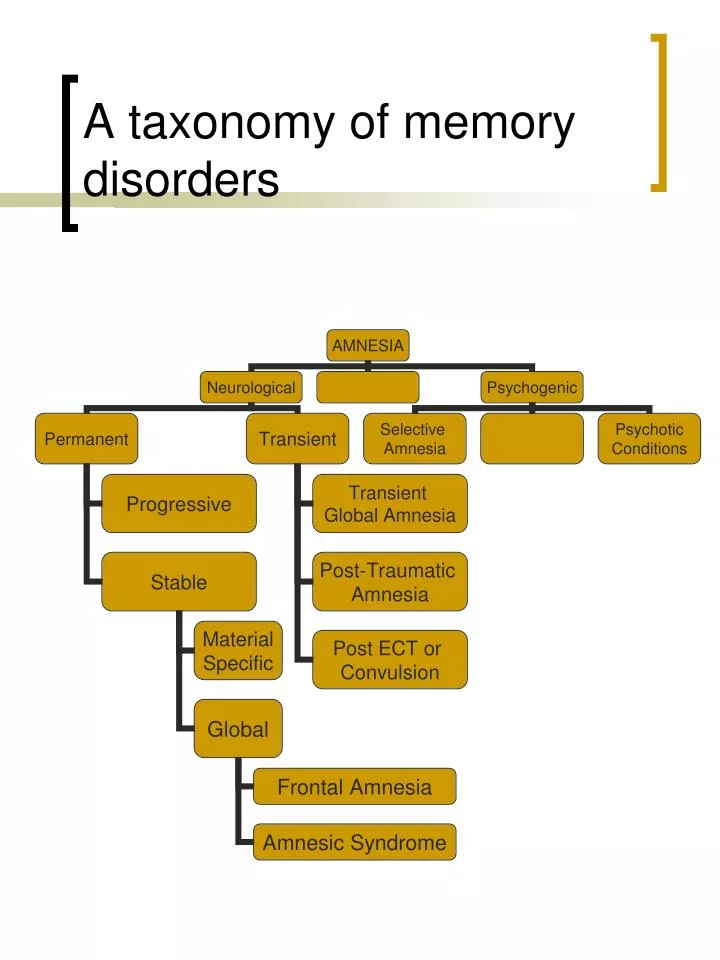
A taxonomy of memory disorders. Cerebral hemispheres. Frontal Amnesia. A. Organisational Deficits Simple registration and recall not affected by frontal lesions Memory problems may be secondary to an inability to organise material for the purpose of committing it to memory

E N D
Frontal Amnesia • A. Organisational Deficits Simple registration and recall not affected by frontal lesions Memory problems may be secondary to an inability to organise material for the purpose of committing it to memory i.e. failure to impose a meaningful structure on the information, to generate appropriate learning strategies Frequent concomitant of traumatic brain injury Manifest on tests such as Rey Complex Figure, Rey Auditory Verbal Learning
Frontal Amnesia • B. Retrieval Problems Retrieval involves strategic problem-solving. Often disturbed following frontal lesions Patient with a retrieval deficit will demonstrate a disturbance of free recall Recognition memory should, however, be intact eg. RAVLT: poor score on recall of list A (trials 1-6) recognition 15/15 One advantage of WMS-III relative to WMS-R
Frontal Amnesia • C. Temporal Discrimination Increasing attention being devoted to this aspect of memory Patients with frontal lesions are markedly impaired in making temporal discriminations. Great difficulty in judging recency and temporal order and in reconstructing sequences. Note, deficits of temporal ordering may be seen in the absence of fontal lobe pathology Two processes involved: • Encoding of information needed for temporal memory • Effective processing of retrieved information regarding temporal order In patients with lesions of the frontal lobes deficit lies in b) ie. Is one of faulty processing (c.f. WKS patients where the deficit lies in a)).
General Amnesic Syndrome • Definition A permanent, stable and global disorder of memory due to organic brain dysfunction which occurs in the absence of any other extensive perceptual or cognitive disturbance. NB. Permanency Stability Pervasiveness Specificity
Clinical Features of the Amnesic Syndrome • Profound difficulty or total inability to acquire new material (anterograde amnesia) • Preservation of immediate memory as measured by tasks such as digit span • Preservation of semantic memory • Preservation of procedural learning • Some retrograde amnesia (variable across patients)
Neuopathology Brain structures implicated: • Bilateral damage to the mesial temporal lobes of both the right and left hemispheres Within these areas the hippocampus has been seen to represent the crucial structure 2. Structures within the diencephalon and specifically: Nuclei within the thalamus Mamillary bodies Mamillo-thalamic tract Fornix All above structures represent part of the limbic system
Aetiology • GAS typically seen in association with • Wernicke-Korsakoff Syndrome • Herpes Simplex Encephalitis • Hypoxia • Anterior Communicating Artery Aneurysm • Thalamic Infarction • Temporal Lobe Resection Other causes: CVA Tumour
Wernicke-Korsakoff Syndrome Typically the result of chronic alcoholism Principle cause: Thiamine deficiency Results in damage to the subcortical structures and in particular the diencephalon Minimal requirement: Lesion of the mamillary bodies and dorsomedial nucleus of the thalamus Typically additional lesions in the frontal lobes (atrophy) due to alcohol neurotoxicity and often the medial temporal structures including the hippocampus Treatment. Thiamine. Amnesia often persists
WKS: Characteristics • Normal memory span • Severe anterograde amnesia • Normal rate of forgetting • Extensive, temporally graded retrograde amnesia • Confabulation present • Cued recall better than spontaneous recall • Recognition relatively intact • Poor at recency judgements • Frontal lobe dysfunction typically present
CASE ST • 49 yo male • Hx: 20 years of heavy alcohol consumption • Dx: WKS • Ax: four weeks after detoxification and thiamine Tx
S.T. • Verbal IQ = 106 • PIQ = 108 • Working Memory = 109 • Processing Speed = 90 • Full Scale IQ = 97 • General Ability = 107
S.T. • INDEX • Auditory Mem = 65 • Visual Mem = 68 • Visual Working Mem = 89 • Immediate Mem = 67 • Delayed Mem = 62
ST • Rey Auditory Verbal Learning Test Trials I-V = 6, 6, 6, 6, 7 Recall B = 5 Recall A = 2 Recognition = 14/15 • Recognition Memory Test Words = Scaled score of 9 Faces = Scaled score of 9 • 15-Item Visual Memory Test Raw Score = 15/15 • COWAT Words = 16 • Wisconsin Card Sorting Test Categories = 2, Perseverative Responses = 83 • Rey Complex Figure
Thalamic Infarction • Primary thalamic haemorrhage relatively frequent, accounting for over 10% if all intracranial haemorrhage. • Amnesia a principle and chronic symptom • Occurrence of thalamic amnesia dependent on infarction occurring in a particular region of the thalamus (dorsomedial nucleus)
Thalamic infarction Amnesia characterised by: • Normal span • Severe anterograde amnesia • RA in majority of cases – no temporal gradient • Confabulation particularly in the early stages post-stroke • May have visuospatial, frontal and language impairments Famous case of NA – Penetrating head injury when fencing foil entered the right nostril, damaging the left thalamus. Demonstrated profound amnesia. RA initially extensive (years) then shrank to weeks. Frequently cited as an example of thalamic damage. However, MRI scanning revealed additional damage to structures including mamillary bodies, mamillo-thalamic tract and anterior (left) temporal lobe.
Anterior Communicating Artery Aneurysm Aneurysm: Localised dilatation of the walls of a blood vessel, usually an artery, due to weakening through infection, injury, degenerative illness or a congenital defect. Rupture frequently associated with a lasting impairment of memory. ACoA particularly prone to the development of saccular aneurysms. Estimated that 30 to 40% of all ruptured aneurysms represent those of the ACoA. ACoA supplies basal forebrain, anterior cingulate, anterior hypothalamus, anterior commissure and the genu of the corpus callosum. Accordingly, frontal lobe damage a frequent concomitant of rupture of the ACoA
ACoA Amnesia Characterised by: • Normal span • Impaired learning (less severely disrupted than in many other conditions) • Facilitated by the provision of strategies suggesting an executive basis • Recognition memory relatively intact • Confabulation present both momentary and fantastic • Impaired temporal discrimination • Typically demonstrate frontal impairments *Group variable in terms of the severity of the memory impairment.
Mesial temporal structures implicated in disorders such as • Herpes Simplex Encephalitis Viral infection causing encephalitis Associated with Type 1 Herpes Simplex (that characterised by the oral lesions) Neuropathology has consistently been reported to principally involve the lateral and medial temporal cortex including the hippocampus after which the virus may extend to the orbito-frontal cortex, the cingulate gyrus and the parietal lobe. Illness initially characterised by an acute confusional state. After this resolves the patient will invariably be left with a severe memory disorder.
HSE amnesia characterised by: • Normal memory span • Profound anterograde amnesia • Rapid forgetting • RA: Variable though usually extensive • Intact implicit memory • Semantic memory deficit
Case PD • 37 yo male • HSE 2 years previously • Currently on pension • Previously manager of a Woolworths store
P.D. Verbal IQ = 112 PIQ = 120 Working Memory = 119 Processing Speed = 115 Full Scale IQ = 117 General Ability = 116
PD • Recognition Memory Test Words = Scaled score of 6 Faces = Scaled score of 5 • Rey Complex Figure Test Copy = 34 Recall = 2.5 • 15-Item Visual Memory Test Raw Score = 10/15
Mesial temporal structures (con’t) 2. Bilateral temporal lobe resection Best known case HM 23 yo man operated on in 1957 by W. Scoville Bilateral resection to control intractable epilepsy. Produced one of the densest amnesias ever recorded
HM’s amnesia characterised by: • Memory span intact • Semantic memory relatively intact • Implicit memory intact • Frontal dysfunction not observed • Profound anterograde amnesia • Anosmic • RA of at least 2 years Other cases of unilateral resection resulting in global amnesia described (presumably pathology on the other side). Typically a unilateral resection will result in a material specific memory disorder
Anoxia Typically secondary to cardiac arrest or the result of carbon monoxide poisoning. Certain cerebral structures are more susceptible to damage than are others. Medial temporal structures (and the hippocampus in particular) are susceptible to damage as are the ‘watershed’ areas of the cortex – areas which lie at junctions between distinct cerebrovascular systems and which are dependent for their blood supply on the most distant radiations of the cerebral arteries.
Transient Memory Disorders Thought to be related to cerebrovascular disturbance (CVD) • Transient Global Amnesia Most commonly reported in association with disturbances of the vertebrobasilar arterial system although has also been reported in association with bilateral MCA disturbance. Patients typically over 50 years and usually experience only one attack (although there have been reports of recurrent episodes) Attacks start suddenly and generally involve: • An inability to form new memories of events experienced during the episode • A temporary amnesia for events in the hours/days preceding the attack • Individual remains alert but perplexed during the episode • Invariably leaves the patient with memory loss for events that occurred during the episode.
2. Transient Ischaemic Attacks (TIA’s) TIA: attack of short-lived focal neurological deficit produced by temporary ischaemia. By definition, recovery should occur within 24 hours. Result of narrowing (stenosis) of an arterial vessel Whether memory impairment evident dependent on site and extent of stenosis
Retrograde Amnesia • Loss of memory or difficulty in recalling events that occurred prior to onset of the amnesia. ??Double dissociation of RA and AA