Download
1 / 11
120 likes | 456 Views
osteomyelitis. kendra morrison em pgy 4 sjhc. etiology. hematogenous seeding monomicrobial ; most common site is metaphysis occurs more commonly in kids (long bones) than adults (vertebrae) contiguous spread of infxn from skin/joints polymicrobial

E N D
osteomyelitis kendramorrison empgy 4 sjhc
etiology • hematogenous seeding • monomicrobial; most common site is metaphysis • occurs more commonly in kids (long bones) than adults (vertebrae) • contiguous spread of infxn from skin/joints • polymicrobial • occurs more in young people (trauma) and older people (decub. ulcers & infected total joints) • direct innoculation from trauma/surgery • polymicrobial • acute vs. chronic
classification • Lee & Waldvogel • based on duration of illness & mechanism • Cierny & Mader • based on affected portion of bone, physiologic status of host & local environment (stage 1-4)
microbiology • staph aureus • coag-neg staph • aerobic gm-neg bacilli • less common • streptococci • enterococci • anaerobes • fungi • mycobacteria
clinical presentation • acute: • gradual onset of sxs (may present as septic arthritis esp. if metaphysis of bone involved is located in joint capsule) (ex: knee, hip, shoulder) • dull pain at site • warmth, erythema & swelling at site • fever +/- rigors • subacute: • pain over several weeks • minimal fever or other constitutional sxs
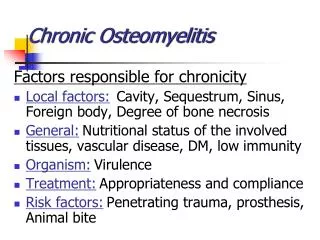
chronic: • pain, erythema, swelling or draining sinus tract (pathognomic) • deep or non-healing ulcers should raise suspicion for osteo (esp. if ulcers lie over bony prominences) • diabetics can present atypically (“2X2”)
diagnosis • bone biopsy to ID pathogen (pos. findings in 87% of cases); do at time of surg. debridement • may not need in setting of pos. blood cxs & pos. radiographic findings • cxs of superficial wounds/sinus tracts do not often yield same causative agent, so not useful • xrays (plain films of affected area) • labs • cbc (leukocytosis in acute but not in chronic) • esr/crp (may be elev. or normal) • blood cxs (more commonly pos. in hematogenous)
treatment • surgical debridement • antimicrobial therapy (table 2) • gm negs = fluoroquinolones • rifampin has activity at the “biofilm” but req. 2nd agent secondary to emerging resistance • hardware removal • hyperbaric oxygen • wound vac