Download

1 / 67
680 likes | 919 Views
Is It Time To Replace Ovarian Stimulation in IVF With Alternatives. Dr. Milton Leong MDCM DSc (McGill) Director, IVF Center , HKSH Specialist in Reproductive Medicine Adjunct Professor, OBS-GYN, McGill University.

E N D
Is It Time To Replace Ovarian Stimulation in IVF With Alternatives Dr. Milton Leong MDCM DSc (McGill) Director, IVF Center, HKSH Specialist in Reproductive Medicine Adjunct Professor, OBS-GYN, McGill University
Drs. Steptoe and Edwards decided to abandon the use of fertility medications and try aspirating a single egg in a natural menstrual cycle. On their second attempt, Louise Brown was conceived The first IVF Baby
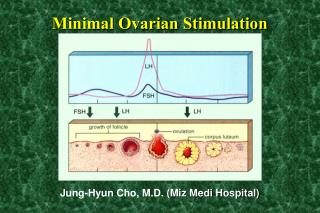
Natural Cycles Clomiphene, Clomiphene/HMG HMG FSH stimulation with agonists FSH stimulation with antagonists Ovarian Stimulation for IVF
WHAT GOES AROUND COMES AROUND *American idiom Ovulation Stimulation
Technology and product development timeline: gonadotrophins r-hFSH FbM Horse PMSG Pig FSH Pituitary FSH u-hMG u-FSH u-FSH r-hFSH (HP) 1930 1940 1950 1960 1980 1990 1995 2003 Consistency Quality Local reactions Potential side-effects Creutzfeldt–Jacobdisease Antibodies Local, systemicreactions Adapted from: Lunenfeld. Reprod Biomed Online 2002;4:11
Poor quality No fertilization or very poor pregnancy rate Cancel egg retrieval Premature LH surge 5-20% 5-20% All cycles treated in early 1980’s
Review “Gold Standard” Discuss Alternatives Introduce Concept of Preparing Ovary for Egg Collection in IVF I
GnRHa Long Protocol vs No Suppressionmeta-analysis IVF cases Odds ratios for IVF clinical pregnancy after GnRH-a versus clomiphene/FSH/hMG ovulation induction protocols
11 patients eligible for IVF GnRH agonists s.c. (busereline) started at day of menstruation of one day before Ovarian stimulation started with HMG or purified FSH when all ovarian follicles and the endometrial lining has disappeared on ultrasound (average 15 days) One ongoing pregnancy achieved Results of first application of GnRH-agonists in the long protocol Porter et al., 1984
FSH with agonist down regulation FSH with antagonists Low dose clomid/FSH stimulation Delayed stimulation IVM Natural cycles OVARIAN STIMULATION
Modifications of natural GnRH to have GnRH agonistic properties 1 2 3 4 5 6 7 8 9 10 pyro (Glu) – His – Trp – Ser – Tyr – Gly – Leu – Arg – Pro – Gly – NH2 regulation of GnRH receptor affinity regulation of biologic activity activation of the GnRH receptor Structure of GnRH agonists
Our contribution to 1. low dose short term agonist downregulation using decapeptyl 2. flexible low dose antagonist Aims: - to simplify treatment - to minimize drug usage Individualizing protocols
Undesirable effects: Over-suppression: LH becomes so low that it affects the production of estrogen, and possibly progesterone in the luteal phase Leads to poor response, poor pregnancy outcome due to early abortion. Also it is: Too long and too much drug use, cost, cancelled cycles and it is unnatural. GnRH agonists
1 2 3 4 5 6 7 8 9 10 pyro (Glu) – His – Trp – Ser – Tyr – Gly – Leu – Arg – Pro – Gly – NH2 regulation of GnRH receptor affinity regulation of biologic activity activation of the GnRH receptor Structure of GnRH antagonists to achieve antagonistic properties of natural GnRH more modifications than only in position 6 and 10 are necessary
Selection Criteria: 1. Previous over-suppression with agonist 2. Previous poor response 3. Previous LH surge if no agonist Cetrorelix 0.125mg Flexible Dose Trial
BMI Distribution Mean = 21.8 (range 19-30)
# Days Cetrorelix Used Mean = 2.2 days (range 1-3)
LH and Cetrorelix 0.125mg/day • Range mIU/ml • Pre 1.2 - 7.8 • Day 1 post 0.9 - 4.9 • Day HCG 1.8 - 6
Conclusions: Why treat 100% of patients when we are trying to prevent 5-10% LH surge Avoid over-suppression and poor response Effective in preventing LH surge Reduction of hyper-stimulation Lower costs The GnRH Antagonists
Cost Physical Suffering Immediate side effects Future side effects OHSS Problems With Ovarian Stimulation
Drug Cost Up to 40% of cost in IVF 30% of patients who would not choose IVF as fertility treatment cited cost as the deciding factor (fertility survey by YWCA HK 2002) Problems with Ovarian Stimulation
In 2 surveys on the population’s perception of IVF, Europe 1996 and Hong Kong 1998, 50% of infertile couples know about IVF but will not undergo treatment. The main reasons are: Religion, Cost, Worried about side effects of drugs
Potential Cancer Risks: Clomiphene use increased risks for Invasive and Borderline epithelial Ovarian tumors Gravid RR 1.4 Nulligravid RR 27.0 Whittemore, Harris et al 1992 Problems with Ovarian Stimulation
OHSS Up to 6% of all FSH stimulated IVF cycles 1.5% Severe Compare NO OHSS with unstimulated cycles Problems With Ovarian Stimulation
Multiple dose protocol rate of OHSS: 6.5% vs. 1.1% (agonist vs. antagonist protocol) RR 6.2, 95% CI: 1.4 - 27.1, p = 0.03 Single dose protocol rate of OHSS: 11.1% vs. 3.5% (agonist vs. antagonist protocol)95% CI: - 18.4 to 3.2 patients requiring hospitalisation: 5.6% vs. 1.8% (agonist vs. antagonist protocol)95% CI: - 11.7 to 4.1 With both Cetrotide protocols a clear reduction of OHSS was achieved Reduction of OHSS using Cetrotide
Waste of Human Resources Excess eggs ? how to deal with Excess embryos - even worse Multiple pregnancies and their associated complications Problems with Ovarian Stimulation
So it is time to Individualise More User Friendly Alternatives
Don’t think STIMULATION Think Preparing the Ovary for Egg Collection Think Patient Orientated Treatment Always Minimise Trauma to Patients New Mindset
FSH/GnRH Down Regulation FSH/GnRH Antagonists Clomid, Clomid/FSH Minimal Stimulation IVM Natural Cycles Ovum Preparation for IVF
Routine IVF Ovulation Stimulation FSH FSH with Agonist Down Regulation FSH with Antagonists Preparation for Egg Collection
Natural Cycle IVF Minimal Stimulation IVF In Vitro Maturation of eggs/IVF Preparation for Egg Collection
We should stop thinking of Ovarian Stimulation, but start to consider, in all IVF cases, that we have to prepare the ovary for egg collection. Only if we do this, we can set our mind on how best we can serve our patients, in their interest and primarily in their interest.
Group A Young age No medical problem or history Previous Pregnancy ANC >5 Consider No Stimulation Preparing the Ovary for Egg Collection for IVF
Group B PCO Previous History of Poor Response Raised Day 2 FSH Consider IVM/IVF with/without stimulation Preparing the Ovary for Egg Collection in IVF
Group C No Contradiction to stimulation No previous Adverse History Normal Day 2 FSH Normal Antral Follicle Count Gold Standard: HMG/FSH with Agonist/Antagonist Preparing the Ovary for Egg Collection
Risk of OHSS Treatment options Cancel cycle Coasting No embryo transfer Convert to IVM Over responders
Prolonged Coasting Aim: To prevent hyperstimulation Practice: Coast till E2 ≤ 3000 pg/mL Sher, 1995 Start when 30% follices > 15 mm Nilsson, 1999 When 3 follicles > 17mm Over responders
A better choice is to convert over-responders, once recognised, to IVM. IN this case, OHSS can be avoided, and pregnancy maintained, as coasting cannot guarantee relief of OHSS, and sometimes oocyte quality is compromised Over Responders
Age (average age of ML patient 38.7 yrs) Decrease ovarian reserve (↑D2 FSH) Decrease antral follicles count Previous ovarian surgery (Laparoscopic ovarian cystectomy) Poor responders