Download
1 / 39
400 likes | 584 Views
Peripheral Nervous System Drugs. Sympathetic: (Adrenergic) Activators Sympthomimetics Agonists Blockers Sympatholytic Antagonists Receptors Alpha 1 & 2 Beta 1 & 2 Dopamine. Parasympathetic (Cholinergic) Activators Parasympathomimetics Agonists Blockers Anticholinergics

E N D
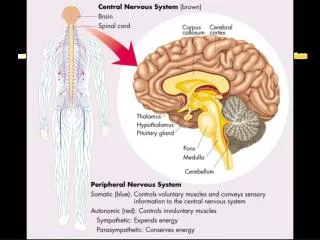
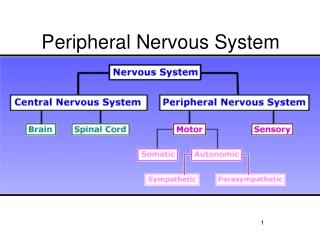
Sympathetic:(Adrenergic) Activators Sympthomimetics Agonists Blockers Sympatholytic Antagonists Receptors Alpha 1 & 2 Beta 1 & 2 Dopamine Parasympathetic(Cholinergic) Activators Parasympathomimetics Agonists Blockers Anticholinergics Antimuscarinics Parasympatholytics Antagonists Receptors Muscarinic Nicotinic N & M **Peripheral Nervous System Vocabulary**
For the Test: Cholinergic Drugs • Muscarinic agonists: no agents • Muscarinic antagonists (anticholinergics): 7 agents see slide • Ganglionic blockers: no agents • Neuromuscular blockers: no agents • Cholinesterase inhibitors: neostigmine, physostigmine (difference and use)
Muscarinic Agonists(Parasympathomimetics) • Limited uses: • Urinary retention • Increase GI peristalsis • Glaucoma, eye surgery • Adverse effects • Bradycardia, hypotension • Excess saliva, cramps, diarrhea • Urinary (contra: bladder obstruction &surgery) • Asthma exacerbation
Muscarinic Poisoning • Sources • Muscarinic agonists • Cholinesterase inhibitors • Mushrooms • Symptoms • Profuse salivation, tearing, bronchospasm, diarrhea, bradycardia, hypotension • Treatment: atropine
Muscarinic Antagonists (Parasympatholytics) • “Anticholinergics” • Agents to know forever • Atropine: strongest, general use • Oxybutinin (Ditropan): overactive bladder • Tolerodine (Detrol): overactive bladder • Scopolamine: sedation, motion sickness • Ipratropium, Tiotropium: lungs • Dicyclomine (Bentyl): IBS, diarrhea
Atropine • Mechanism: blocks muscarinic receptors by competing with Acetylcholine • high doses will block nicotinic as well • Route: PO, topically (eye), injection
Pharmacologic effects: ↑ heart rate ↓ secretions (GI, tear, salivary) ↓ smooth muscle (peristalsis, urination) Dilate eye (mydriasis) ↑ CNS excitability Therapeutic Uses Preanesthesia (make sure heart doesn’t stop) Eye surgery: (dilate eye) Bradycardia: ↑ heart rate Intestinal hypertonicity, hypermotility (slows GI tract) Muscarinic Agonist Poisoning (antidote) Atropine
Adverse (Anticholinergic) EffectsMust Know: “Just too much effect” • Xerostomia (Dry Mouth) • Blurred vision, photophobia • Elevation of IOP • Urinary retention • Constipation • Anhidrosis (no sweat) • Tachycardia • Asthma: secretions too thick and crusty • Dementia
Anticholinergic Toxicity • Dry as a bone • Red as a beat • Hot as a hare • Blind as a bat • Mad as a hatter • **Must determine whether psychosis is real or anticholinergic • Treatment: • Minimize absorption • Cholinesterase inhibitor
Dose dependent Low dose High dose Glands: sweat, salivary, bronchial Heart Eye Bladder Intestine motility Lung Stomach Atropine
Interactions • Drugs with anti-muscarinic (anticholinergic) side effects effects • Antihistamines • Phenothiazine antipsychotics • Tricyclic antidepressants • Furosemide (Lasix)
Cholinesterase Inhibitors(Parasympathetic Agonists) • Increase Acetylcholine at all receptors! • Reversible (must know these agents) • Neostigmine: myasthenia gravis • Physostigmine: anti-cholinergic antidote • Irreversible (do not need to know for test) • Used as insecticides • Developed in WW2 as “nerve gas” • One is used for glaucoma (just trivia for you attorney types)
Myasthenia Gravis • Etiology: Antibodies against Nicotinic-M receptors • Clinical manifestations: fatigue, muscular weakness, dyspnea • Treatment • Cholinesterase inhibitors • Side effects: can cause accumulation of acetylcholine and nicotinic-M and muscarinic receptors
Myasthenia Gravis • Treatment • Side effects cont • Muscarinic effects • Neuromuscular blockade (toxicity)
Neuromuscular Blockers • Neuromuscular Blockers • Paralyze muscle • Use to intubate so they don’t fight • Agents • Nondepolarizing: tubocurarine, et al. • Depolarizing: succinylcholine • Uses • Surgery • Mechanical Ventilation, ET intubation • Adjunct to ECT
Adrenergic Drugs • Phenylephrine and Pseudoephedrine • Epinephrine, Norepi, Dopamine, Dobutamine • All lung beta-2 agonists • Alpha blockers: terazosin, phentolamine • Beta blockers: propanolol, metoprolol, atenolol, carvedilol • Indirect antagonists: Clonidine
Catecholamines: Broken down by MAO and COMT in liver and intestine Parenteral only Cannot be given orally, short half-life Colorless solutions; color is sign of oxidation Natural catecholamines: epi, norepi, dopamine Synthetic: dobutamine (others we don’t need to know) Non-catecholamines Can be given PO Last longer in body Adrenergic Agonists Activate alpha and beta receptors
Adrenergic Agonists • Noncatecholamines • Phenylephrine: (alpha1) nasal congestion, inotropic support (rare now) • Pseudoephedrine (all alpha and beta): • Nasal congestion • Can be used to make amphetamines
Alpha1 Activation • Therapeutic effects • Vasoconstriction • ↑ BP (intensive care, last resort) • Hemostasis • ↓ local anesthesia absorption • ↓Nasal decongestion • Mydriasis • Adverse effects • Hypertension • Necrosis • Bradycardia
Beta1 Activation • Therapeutic Uses • Cardiac arrest (make heart beat again) • Heart Failure: inotropic support • Shock: inotropic and chronotropic support • A-V heart block (speed conductivity) • Adverse effects • ↑ HR • Angina pectoris • dysrhythmia
Beta2 activation • Therapeutic use • Asthma: bronchodilate • Preterm labor: stop contraction • Adverse effects • Hyperglycemia • Tremor
Therapeutic uses: ↓ absorption of local anesthetics Control superficial bleeding ↑ BP Mydriasis AV block, V. fib, Asystole Status Asthmaticus Anaphylactic shock Reduce nasal congestion Adverse events Hypertensive crisis Dysrythmias Angina pectoris Necrosis Hyperglycemia EpinephrineReceptors: all alpha and beta
Epinephrine • Absorption • Inhalation: minimal • Injection • Preparations • SC, IM, IV, Intracardiac, intraspinal, inhalation, • Lidocaine with epi • No fingers, nose, penis, and toes • Inactivation: MAO and COMT in liver
Epinephrine • Interactions • MAO inhibitors (why oh why?) • Alpha-adrenergic blocking agents • Beta-adrenergic blocking agents
Dopamine • Receptor: dopamine, alpha1, (beta1 higher doses) • Therapeutic Uses • Shock: • ↑ HR and contractility • Maintain renal artery perfusion • Heart failure: same as above • ARF: low dose (may not be effective) • Adverse Effects • Dysrhythmias, angina pectoris
Beta-2 agonists • Short acting • Albuterol • Levalbuterol • Long acting • Salmeterol • Formoterol
Other Adrenergic Agonists • Dobutamine (beta1) uses • Shock (inotropic support) • Stress Echoes • Terbutaline: (beta2) uses • Stop preterm labor contractions
Norepinephrine • Receptor: alpha 1 & 2, beta1 • Therapeutic uses • Hypotensive state • Cardiac arrest (last resort) • Brand: Levophed (Leave ‘em dead!)
Adrenergic Antagonists Can be quite selective for receptors
Therapeutic uses Hypertension BPH Reverse toxicity of epinephrine Pheochromocytoma(what is it?) Raynaud’s disease Adverse effects Orthostatic hypotension Reflex tachycardia Nasal Congestion Inhibition of ejaculation Na+ & H2O retention Alpha1-blockers
Alpha-Adrenergic Blockers • Prazosin - HTN • Doxazosin – HTN, BPH • Terazosin – HTN, BPH • Tamsulosin – BPH • Phentolamine – Pheochromocytoma, tissue necrosis
Therapeutic Uses MI HF Angina Pectoris Dysrhythmias HTN Other Hyperthyroid Migraine Stage Fright Pheochromocytoma Glaucoma Adverse Effects (β1) ↓ HR CO AV heart block Precipitate HF Rebound cardiac excitation Adverse Effects (β2) Bronchoconstriction Inhibition of glycogenolysis Beta-blockers
Beta1, Beta2 Propanolol* Nadolol Pindolol Selective Metoprolol* Atenolol* Bisoprolol * Means must know Beta1,beta2, alpha1 Labetalol Carvedilol* Used for HF Metoprolol* Carvedilol* Beta Blockers Agentsby receptor selectivity
Indirect Adrenergic Antagonists • Clonidine • activates alpha-2 receptors in CNS ↓ norepinephrine release • Uses • Hypertension • Pain relief in cancer (epdidural use only) • Adverse effects • Drowsiness, dry mouth, rebound HTN, bradycardia • Preparations • Oral: at least twice a day • Transdermal: seven days
Indirect Adrenergic Antagonists • Reserpine • Suppresses NE synthesis and promotes MAO-mediated destruction • Crosses BBB • Effects • Hypotension • Adverse effects • Depression, sedation, apathy • Bradycardia, hypotension • Guanethidine: similar but fewer CNS effect
Indirect Adrenergic Antagonists • Methyldopa, Methyldopate • Similar to clonidine, but are taken up in brain stem neurons and converted to active alpha2 agonist • Use: HTN • Adverse effects • 10 – 20% Positive Coombs test (5%) will go on to have hemolytic anemia • Hepatotoxicity • Drowsiness, dry mouth, hypotension, etc.