Download
1 / 29
290 likes | 405 Views
Additional Case 1. Presentation to GP. David, 21, apprentice plumber R leg injury during rugby game (last pm) Hit from R side during tackle Impact on upper outside 1/3 of leg (foot planted on ground) No previous Hx of knee injuries No PMH of note. Review the anatomy of the knee.

E N D
Presentation to GP David, 21, apprentice plumber R leg injury during rugby game (last pm) Hit from R side during tackle Impact on upper outside 1/3 of leg (foot planted on ground) No previous Hx of knee injuries No PMH of note
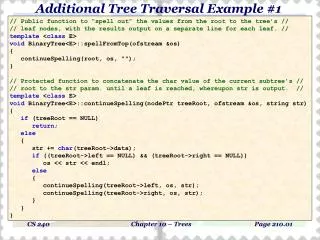
Review the anatomy of the knee Tubercle Epicondyle Condyle Condyle Articulation Articulation Condyle Tubercle
What is the functional role of the major ligaments of the knee? Patellar ligament: makes up the joint capsule on either side of the patella; maintains patella alignment Collateral ligaments: contribute to stability when standing (this is when they are taut) are also ‘check’ ligaments for flexed rotation (permit but limit rotation) Oblique popliteal ligament: reinforces the joint capsule posteriorly Arcuatepopliteal ligament: strengthens the joint capsule posterolaterally Anterior cruciate ligament: limits posterior rolling of the femoral condyles on the tibial plateau during flexion; prevents posterior displacement of the femur on the tibia and hyperextension of the knee joint Posterior cruciate ligament: limits anterior rolling of the femur on the tibial plateau during extension; also prevents anterior displacement of the femur on the tibia and helps prevent hyperflexion of the knee joint.
Based upon the mechanism described, which structure/s are likely to be injured? ACL Medial collateral ligament tear
What are the typical mechanisms which lead to injury to the major ligaments and menisci? ACL: Non-contact change of direction; hyperextension on landing from a jump or; direct valgus force PCL: Contact injury to the ground or; clash of knees MCL: Contact valgus injury Meniscal tears: Twisting on a planted foot
Examination Positive swipe test Tenderness along the subcutaneous border of the fibula (around the area he identifies as the impact site) Grade 3 laxity with valgus stress Lachman’s Test and anterior draw are inhibited by pain from David
Initial management Tell David he has injured a major knee ligament and that the pain is from local bruising Knee splint + crutches Refer for physiotherapy rehab and advice on weight bearing/return to work+sport
Review the knee examination and the pathology which each special test is aimed at demonstrating • Look: • Swelling, wasting, spasm, scars, erythema, deformities • Posture (leg length, foot posture) • Gait (walk 10 steps, in/out of chair, socks on/off) • Feel: • Skin: temperature • Quadriceps bulk (loss of tone/bulk, spasm, tenderness, loss of continuity in extension) • patella (tenderness, thickened ligament, gaps, creptius, articular surface, suprapatellar bursa, prepatellar bursa) • Medial/lateral femoral condyles and epicondyles • Medial and lateral colateral ligaments • Medial and lateral joint lines • Poplitealfossa (masses, pulse)
Knee effusion: is the swelling within joint or extrinsic to joint? • Patella tap: slide hand down thigh towards knee; push down gently on patella • Swipe/bulge test: stroke medial side upwards; empty suprapatellar pouch; stroke lateral side downwards • Move: • Flexion: 135⁰; extension: 0-10⁰ • Observe patellar tracking • Special tests • Patella apprehension: patella dislocation (knee flexed 30⁰; thumbs on medial border; lateral force) • MCL/LCL stress test: MCL/LCL tear (knee flexed 15-30⁰; varus/valgus force to distal tibia; repeat in full extension) • Anterior draw test: ACL tear (knee flexed; sit on foot; gently pull upper tibia forwards) • Lachman’s test: ACL tear (knee slightly flexed; stabilise femur with hand; apply pressure to posterior proximal tibia to move it anteriorly) • McMurray’s test: medial/lateral meniscal tear (full flexion; externally rotate foot + varus force Vs internally rotate foot + valgus force; extend knee
What is the effect of muscle inhibition and spasm on ligament testing ? Source: Angus Hann With Ligament testing you assess symptom response ( pain), laxity and end feel. Acute spasm will guard the joint and give u a false negative on Ligament testing. Inhibition affects strength. May be unable to straight leg raise. Pain causes reflexive inhibition and may cause knee to give way. Need to encourage patient to relax when testing. Acute knee difficult.
3. What could be done to improve your confidence in the Lachman's and anterior draw test in this case? • Tell the patient to relax and practice more • UptoDate: The stability of the knee is assessed by varus and valgus stress testing, the Lachman's test, and the anterior and posterior drawer signs. The usefulness of these tests is limited if the patient's muscles are not relaxed, as quadriceps contraction masks signs of instability • To improve confidence – be Angus or Pete
4. What happens to the quadriceps muscle group with knee injury and splinting, does it matter? - what proactive measures may limit or prevent this? • Rupture – patella loses its anchor patella moves inferiorly (towards foot) unable to straighten knee • A large sudden load may cause the entire insertion to be compromised, leading to complete rupture. Repetitive loading, particularly eccentric loads, causes microfailure, usually at the muscle tendon junction. This microfailure can result in partial tears • Strain – due to repetitive functional overload, knees subjected to high levels of repeated loading of extensor mechanism
Trigger 3 The following week you are surprised to see David represent with a letter from the physio agreeing with your diagnosis about the knee injury, but expressing concern about the cause of the ongoing leg pain. Repeat clinical examination shows a large effusion and there is laxity with Lachman's test. You refer David for an x-ray which is shown below.
Describe the anatomy seen on the x-ray image. Femortibial joint space Fibula Head Neck Body
Describe any visible pathology on the x-ray image. hyper-extension lateral view allows assessment of slope of intercondylar roof in relation to the tibial plateau; Plain radiographs cannot be used to diagnose ACL tears. In some cases, an avulsion fracture of the anterolateraltibial plateau (ie, Segond fracture) is identified at the site of attachment of the lateral capsular ligament.
3. Review the mechanism of injury and describe the sequence of events that occurred to his knee. The impact was on the upper outside one third of the leg while his foot was planted on the ground. running landing from a jump
1. What is the common mechanism for ACL rupture? A blow to the side of the knee, which can occur during a football tackle, may result in an ACL tear. Coming to a quick stop, combined with a direction change while running, pivoting, landing from a jump, or overextending the knee joint (called hyperextended knee), also can cause injury to the ACL. Basketball, football, soccer, and skiing are common causes of ACL tears
2. ACL ruptures in children are uncommon - why? - What injury might a child sustain instead? The ACL infrequently ruptures in children. Rather the bone on either end comes off.
4. What are the potential long term sequelae to an ACL rupture which is not operated on in this age group? Depends on activity level of patient Long term sequelae include instability, particularly with pivoting type sports, but even walking Instability causes damage to the menisci and the other ligaments


![CASE STUDY ASSIGNMENT [Additional Guidance]](https://cdn1.slideserve.com/2972132/slide1-dt.jpg)