Download
1 / 35
350 likes | 486 Views
Webinar: Challenges in Clinical Training Ben Wallace, Executive Director, Clinical Training Reform Health Workforce Australia. Health Workforce Australia. Federal government authority

E N D
Webinar: Challenges in Clinical Training Ben Wallace, Executive Director, Clinical Training Reform Health Workforce Australia
Health Workforce Australia Federal government authority Established in 2010 following agreement from federal and state/territory governments that large scale workforce reform is necessary Aims to build a sustainable health workforce that meets the health care needs of all Australians Focus on linking the efforts of health and higher education sectors
International Context: Human Resources for Health Source: World Health Organization, The world health report 2006: working together for health Global shortages of health workers
International Context: Growth in Health Expenditure Source: The World Bank 2014, http://data.worldbank.org/indicator/SH.XPD.TOTL.ZS
International Challenges: Human Resources for Health • Most countries are experiencing a rapid growth in health expenditure and increasing demand for health workforce. • Drivers of change vary, but the challenges of; effective governance of health profession education, effective workforce planning, maximising training efficiency and effectiveness appear common • Complex challenges, including: • Supply and demand discrepancies • International labour flows • Ageing populations (for some) • Geographic distribution
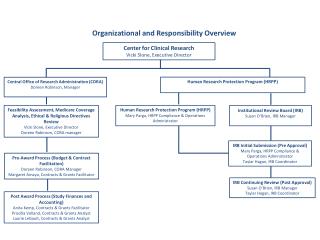
Health Workforce Governance Health profession training involves a large number of stakeholders In many countries, responsibility for health profession training is split across health and education Ministries In many countries high level planning is made more difficult by regional dimensions and by complex funding models for both education and health service delivery. Change is complex and requires political commitment and stakeholder collaboration
Stakeholders needed to reform and expand health professional education Source: World Health Organization 2011, Transformative scale up of health professional education
Australia: National Medical Training Advisory Network (NMTAN) Better alignment of medical training with workforce need by bringing together wide range of stakeholders The NMTAN will produce five-year rolling medical training plans across the whole medical training pipeline The national medical training plan will provide target ranges for training in relation to medical students, interns, basic and advanced trainees Agreement from sector of an urgent need to have better coordination of medical training to meeting current and future workforce
Key discussion questions What mechanisms exist to support health workforce planning in countries in the region? What approaches have been taken to bring together health and education sectors to plan for the future? What possibilities exist for regional learning/cooperation?
Workforce Planning Example: Nursing HWA has built a stock and flow model to estimate future supply and demand for the health workforce HWAhas used a scenario modeling approach to workforce planning which allows policy makers to understand the likely outcomes if no action is taken, and then to see the impact of a range of possible policy interventions. The next two slides show the outcomes of current scenario modeling for the nursing workforce.
Nurse Workforce Planning: impacts of supply and demand measures Working example only – Not for further distribution
Nursing workforce planning: combined scenario results Working example only – not for further distribution
Requirements for planning Sound data sources Effective stakeholder engagement Consensus building on key assumptions
Discussion questions What approaches have other countries taken to workforce planning? What are the strengths and weaknesses of different approaches? How have stakeholders been engaged in the planning process? What scope is there for collaboration in the region?
Efficiency of Clinical Training In Australia, national registration and accreditation bodies prescribe the number of clinical training hours and determine if and how simulation can be included There are large variances in course length and clinical training times There is relatively little evidence about the impacts of these variances on attainment of competency There are a mixture of time based and competency based approaches to accreditation
Clinical Training Profile: Physiotherapy Range of clinical training hours across physiotherapy programs, 2012 Source: Health Workforce Australia survey of 2012 clinical training placements
Key issues/discussion questions What are the variances in length of training in your country? Could health professionals be trained more quickly? What further evidence is required regarding competency based approaches? What is the balance of responsibility between educators and employers in preparing a new professional for practice?
Can Simulation Improve Training Efficiency? Simulated learning environments can provide a realistic and flexible alternative to traditional clinical training and can reduce the strain on clinical training providers
Embedding Simulation in Clinical Training in Physiotherapy • Aims to develop, implement and evaluate, on a national level, a model to substitute simulation for relevant, traditional clinical placement training experience in the training of professional entry students in Physiotherapy programs with full accreditation • Outcomes of Phase 1 • Support from 16 accredited programs • Support from accreditation body • Development of three models of simulation for adoption • Agreed evaluation plan
Embedding Simulation in Clinical Training in Physiotherapy Progress of Phase 2 16 accredited physiotherapy programs implementing the partial substitution model in 2014 and 2015 40 simulation scenarios across three core physiotherapy practice areas have been developed, including supporting documents and videos to train simulated patients Participating sites have received simulation equipment, resources and training to staff to improve simulation capacity By early 2015, over 1700 professional entry physiotherapy students will have completed a clinical placement using the partial substitution model.
Key Issues/Discussion questions Two key questions: What combination of simulation and on-the-job training is most effective? What is the most cost-effective way of implementing simulated learning environments?
Distribution of clinical training Training has traditionally been highly concentrated in: public hospitals acute sector metropolitan locations; This has left other settings (private, community, primary care, aged care, rural) under-utilised as a source of training capacity.
Acute settings56% Public providers71%
Distribution of clinical training Rural and Remote7 % Broadening training in the locations in which we need workforce in the future may have the additional benefit of assisting in workforce distribution
Key issues/discussion questions Many countries are experiencing workforce capacity and distribution issues Can location of training influence workforce distribution? How can we better prepare our workforce for future roles?
Global challenges • Health Workforce Planning Approaches • Health Workforce Governance • Using Training to better distribute the workforce • Balancing health education efficiency and effectiveness. • Outcome and/or compliance focus • Time based and/or competency based • Length and nature of clinical exposure • Length, timing, blend of simulated learning environments • Supervisor training and support