Download
1 / 153
1.68k likes | 2.24k Views
SCREENING. Dr. Aliya Hisam Community Medicine Dept. Army Medical College, RWP. Learning Objectives. Screening Test Aims & Objectives Types , uses and cut-off point Wilsons Criteria To be able to construct a 2 * 2 table.

E N D
SCREENING Dr. Aliya Hisam Community Medicine Dept. Army Medical College, RWP
Learning Objectives • Screening Test • Aims & Objectives • Types , uses and cut-off point • Wilsons Criteria • To be able to construct a 2 * 2 table. • To be able to evaluate screening test and Interpret result in words.
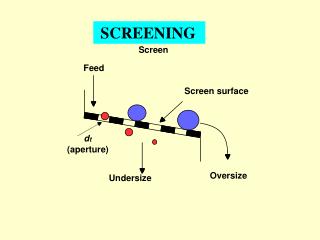
Screening Definition:- “The presumptive identification of unrecognized diseases or defect by the application of tests, examinations or other procedures which can be applied rapidly to sort out apparently well persons who probably have a disease from those who probably do not.”
SCREENING • Application of a test • to asymptomatic people • to classifying them • into diseased or non-disease ppl.
The screening test itself does not necessarily diagnose illness, those who test positive are evaluated by a subsequent diagnostic procedure to determine whether they in fact do or do not have the disease
Aims & Objectives of Screening • It is carried out in a hope that earlier diagnosis and subsequent treatment favorably alters the natural history of the disease in a significant proportion of those who are identified as positives
Iceberg Phenomenon of Disease • Submerge portion:- • Hidden mass of the disease (e.g. subclinical cases, carriers, undiagnosed cases). • Floating tip:- • What the physician sees in his practice.
Types Of Screening • Mass • Multiple or multiphasic • Targeted • Case finding or opportunistic
Uses of Screening • Case detection • Control of disease • Research purpose • Educational opportunities
Model for early detection programmes Disease onset detection First Possible Point Final Critical Diagnosis Usual Time of Diagnosis Outcome Cured/Death Screening Time Lead Time Lag Time
Errors in evaluation of Screening Tests • An error in the evaluation of a screening test, known as lead time bias, can occur when persons with disease detected by screening appear to live longer simply because of the earlier recognition of their illnesses. • An error in the evolution of a screening test, known as length-biased sampling, can occur when persons with disease detected by screening appear to live longer simply because they have more slowly progressing illnesses.
Criteria of Screening • Depends on two consideration:- • Disease • Screening Test
Disease appropriate for screening(Wilson’s Criteria) • Disease should be serious • Screening may help in the prevention of transmission of disease • Prevalence of pre-clinical disease should be high. • Early asymptomatic stage.
The Disease natural history should be adequately understood • Facilities should be available for confirmation of the diagnosis. • There is an effective treatment. • There should be an agreed-on policy concerning whom to treat as patients • Treatment reduces morbidity and mortality. • The expected benefits of early detection exceed the risks and costs. • Done as a regular and on-going process.
Acceptability Validity (accuracy) Sensitivity Specificity Yield + predictive value - predictive value Simplicity Safety Rapidity Ease of admin. Cost Repeatability Screening Test Criteria:-
Validityof a screening test is measured by its ability to do what it is supposed to do i.e., provides a good preliminary indication of which individuals actually have the disease and which do not. • Validity has two components: • Sensitivity • Specificity
Sensitivityof a test is the ability of the test to detect disease in all those who actually have the disease (i.e., correctly identify all those who have the disease) • Specificityof a test is the ability of the test to rule out disease in all those in whom the disease is actually absent (i.e., correctly identify all those who do not have the disease).
PATHOGENESIS C A B D Disease detectable By screening Symptoms develop Cured/Death Biologic Onset Detectable preclinical phase Detectable preclinical phase in natural history of diseases
Sensitivity and Specificity at Different screening Test values Distribution of cases and no cases by screening test values Value chosen to Define a “positive” Screening result 0 =non-cases =cases 0 0 0 0 0 0 Number of persons 0 0 0 0 0 0 0 x x 0 0 x x x x x x x x Test Result 100 110 115 120 130 140 90
Below Point A: Very low range of test results indicate absence of disease with very high probability, • Above Point B : Very high range that indicates the presence of disease with very high probability. • However, where the distributions overlap, there is a "gray zone" in which there is much less certainly about the results.
If we move the cut-off to the left, we can increase the sensitivity, but the specificity will be worse. • If we move the cut-off to the right, the specificity will improve, but the sensitivity will be worse. • Altering the cut-off point/criterion for a positive test will always influence both the sensitivity and specificity of the test.
Sick people incorrectly identified as healthy Healthy people incorrectly identified as sick
Yield of a screening test is the number of persons detected by a screening program. • It is an important measure for determining the usefulness of a test under field conditions. • Positive Predictive Value • Negative Predictive Value
Positive predictive value (PV+) is the proportion of positive tests in people with disease. • Negative predictive value (PV-) is the proportion of negative tests in people without disease.
Sensitivity ? Specificity + Predictive Value - Predictive Value
Sensitivity Proportion of people with disease having + test result. Specificity ? + Predictive Value - Predictive Value
Sensitivity Proportion of people with disease having + test result. Specificity Proportion of people without disease having – test result + Predictive Value ? - Predictive Value
Sensitivity Proportion of people with disease having + test result. Specificity Proportion of people without disease having – test result + Predictive Value Proportion of + test results in people with disease - Predictive Value ?
Sensitivity Proportion of people with disease having + test result. Specificity Proportion of people without disease having – test result + Predictive Value Proportion of + test results in people with disease - Predictive Value Proportion of – test result in people without disease
Disease Yes No Test Result a + b ? a b Positive c + d ? Negative c d a + c ? b + d ? a + b + c + d
Disease Yes No Test Result a + b ? a b Positive c + d ? Negative c d a + c b + d a + b + c + d All those who actually have the disease. All those who actually do not have the disease
Disease Yes No Test |Result a + b a b All those who test + on ST Positive c + d Negative c d All those who test - on ST a + c b + d a + b + c + d
Validity • An ideal screening test is one that is 100% sensitive and 100% specific. • In practice this does not occur.
If disease is present an ideal, or truly accurate, test will always give a positive result. • If disease is not present, the test will always give a negative result. • But this is not the case….
In a 100 group of population, • 60 have disease • 40 do not have disease