Download
1 / 27
290 likes | 530 Views
Clinical Pathology Haematology Case E. Ainsley McDonald Veronica Nou Poonam Shrestha Mary Tormey. Ms SP, aged 25, has been taking clozapine for 6 months. What is agranulocytosis? Explain what haematological parameters must a pharmacist sight before dispensing clozapine.

E N D
Clinical Pathology Haematology Case E Ainsley McDonald Veronica Nou Poonam Shrestha Mary Tormey
Ms SP, aged 25, has been taking clozapine for 6 months. • What is agranulocytosis? • Explain what haematological parameters must a pharmacist sight before dispensing clozapine. • What other haematological ADRs are associated with clozapine? • Explain whether the same monitoring is required for olanzapine.
What Is Agranulocytosis? • A condition in which there is an insufficient number of white blood cells called neutrophils or granulocytes. • This can be caused by • a failure of the bone marrow to make sufficient neutrophils or • when white blood cells are destroyed faster than they can be produced. • Granulocytopenia; Granulopenia; Neutropenia
Granulocytes are a type of white blood cell. When they are examined under a microscope, they appear to contain granules, or small dark specks. • Neutrophils, basophils, and eosinophils are all types of granulocytes. • These cells are important in the immune system meaning affected people are more susceptible to infections.
What is going on in the body? • The bone marrow contains special cells known as stem cells. • Stem cells may develop into red blood cells, white blood cells, and platelets. • Certain conditions can damage stem cells, or change their environment causing them to stop production. • This may cause a low level of granulocytes in the body or agranulocytosis.
What are the signs and symptoms of the condition? • Someone who has agranulocytosis may develop life-threatening or chronic infections. • Symptoms vary, depending on the type of infection, but may include the following: • Chills • Fever • Sore throat • Ulcers in the mouth, stomach or bowels • Weakness
What are the causes and risks of the condition? • Agranulocytosis can be caused by a number of factors, including: • Autoimmune disorders, or conditions in which the body attacks its own tissues • Chemotherapy • diseases that damage the bone marrow • hereditary disorders • radiation therapy • Certain medications, such as clozapine or carbamazepine
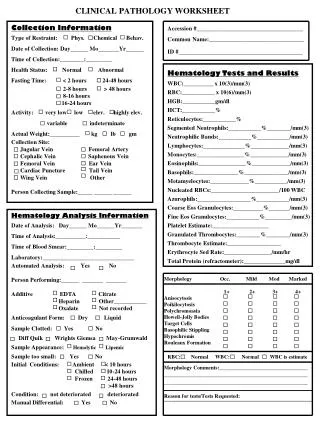
How is the condition diagnosed? • Diagnosis is usually conducted using a complete blood count, or CBC, to measure the level of neutrophils, basophils, and eosinophils. • Genetic testing may be done if heredity is suspected to be the cause. • If blood tests are abnormal, the provider may order a bone marrow biopsy. This test involves inserting a special needle into the hip bone. A sample is taken from the bone marrow.
What are the long-term effects of the condition? • Agranulocytosis increases a person's risk for infections. If white blood cell levels are extremely low, serious bacterial infections can occur. • Can include infections caused by bacteria that usually don't cause any problems in the body. • Infection in the bloodstream, known as sepsis, may lead to life-threatening septic shock. • Increased risk for chronic infections. These can cause organ damage and scarring.
What are the treatments for the condition? • Initial treatment of agranulocytosis often includes the following: • antibiotics to treat or prevent infections • isolation to keep the person from contracting an infection • stopping the medication that is suspected as the cause of the agranulocytosis, which may resolve the problem • Other treatments may be ordered, depending on the cause of the agranulocytosis. These treatments include: • bone marrow transplant • granulocyte-colony-stimulating factors, such as GM-CSFs or G-CSFs, which stimulate the production of granulocytes • matched stem cell transfusions, which replace damaged stem cells
Bone marrow transplant is an effective treatment for some people with agranulocytosis. • More than half of good candidates for bone marrow transplant are cured. • People are good candidates if they meet these criteria: • under the age of 40 years. • good health prior to the transplant. • matched donor, such as a family member.
What happens after treatment for the condition? • Until blood cell counts return to normal, someone who has agranulocytosis is at risk for infection. • Important to avoid risk factors, such as the following: • activities that cause a rapid heartbeat, chest pain, or shortness of breath • excessive exercise • exposure to contagious diseases
What is Clozapine? • Atypical Anti-psychotic. • Used in the treatment of Schizophrenia in patients who have had an inadequate response to at least two other anti-psychotics, or who cannot tolerate the side effects of these.
Warning! • Clozpine can cause agranulocytosis. (Usually reversible on withdrawal of the drug, although can be fatal) • Only patients that have an initial leucocyte count (WBC > 3500mm3 and normal differential blood count) can commence treatment. • This blood test must be performed 10 days prior to starting treatment.
Monitoring • Regular WBC counts and absolute neutrophil counts: • Weekly during the first 18 weeks • At least monthly thereafter • AND for 1 month after complete discontinuation of treatment.
Monitoring (2) • At each check-up flu- like symptoms should be reported (fever, sore- throat) as could be a sign of neutropenia. • An immediate differential blood count must be performed if patient shows signs of illness.
Haematological ADRs associated with Clozapine • Granulocytopenia and Agranulocytosis • Granulocytopenia is defined as a reduced number of blood granulocytes, namely neutrophils, eosinophils, and basophils • Agranulocytosis can prove fatal • Occur within the first 18 weeks of treatment • Withdrawal of the drug is required
Haematological ADRs associated with Clozapine • Leucocytosis and Eosinophilia • in the initial weeks of treatment • Discontinuation of therapy may be warranted in the event of eosinophilia • Discontinue Clozapine if the eosinophil count rises above 3,000/mm3, and to restart therapy only after the eosinophil count has fallen below 1,000/mm3
Haematological ADRs associated with Clozapine • Thrombocytopenia has been reported rarely • reduction in the number of platelets in the blood • results in bleeding into the skin, spontaneous bruising , and prolonged bleeding after injury • recommended to discontinue Clozapine if the platelet count falls below 50,000/mm3
Explain whether the same monitoring is required for olanzapine.
olanzapine • Also an atypical antipsychotic - but of lower efficacy than clozapine • Not associated with agranulocytosis, whereas clozapine has a 1% incidence (TG-P p2) • The only common hematological disturbance associated with olanzapine in clinical trials was eosinophilia (eMims2003) • Rare adverse effect neutropenia (AMH 2003), whereas clozapine has a 2-3 % incidence
olanzapine • Post Marketing surveillance::(APPG 2002) • Hematological adverse effects: • Leucopenia - rare (0.1-0.01%) • Thrombocytopenia - very rare (<0.01%)
olanzapine • Hyperglyceamia may occur in patients who had random BGL at the upper limit of normal - • Check glucose tolerance in patients who gain weight • Increased risk of developing type 2 diabetes while taking olanzapine
olanzapine • For all antipsychotics::(AMH 2003 p669) • Routine FBCs & LFTs are advisable, particularly during the first few months of treatment and are mandatory with clozapine • Monitor weight gain, blood glucose & cholesterol