Download
1 / 42
430 likes | 599 Views
Childhood cancer in Africa French African Pediatric Oncology Group experience. Mhamed Harif CHU Mohammed VI, Marrakech, Morocco m.harif@menara.ma. Africa. Continent Size: 30,065,000 sq km. Population: 1,000,000,000 (2009) < 15 years : 500 M. (2009). More than 50 000 cancers

E N D
Childhood cancer in AfricaFrench African Pediatric Oncology Group experience Mhamed Harif CHU Mohammed VI, Marrakech, Morocco m.harif@menara.ma
Africa Continent Size: 30,065,000 sq km • Population: • 1,000,000,000 (2009) • < 15 years : • 500 M. (2009) More than 50 000 cancers expected in children each year
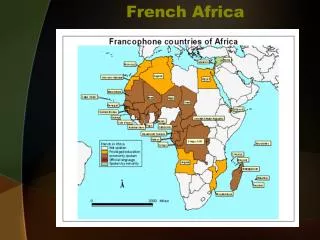
GFAOP EN 2000 8 Unités pilotes 6 pays africains Algerie : Algiers Oran Cameroon : Yaoundé Madagascar : Antananarivo Maroc : Rabat Casablanca Senegal : Dakar Tunisie : Tunis
Pediatric Oncology Units involved 2010 • North Africa • Tunisia 1 unit • Algeria 2 units • Morocco 2 units • West Africa • Senegal 1 unit • Ivory Coast 1 unit • Mali 1 unit • Burkina Faso 1 unit • Togo 1 unit • Central Africa • Cameroon 1 unit • Congo 1 unit • Madagascar • Antananarivo 1 unit • 13 Units French Speaking Africa
French-African Paediatric Oncology GroupGFAOP ------- Created in April 2000 ------- • Objective : • Improve the management of childhood cancer in Africa • Setting up a database of pediatric cancer in Africa • Methods : • Teaching and training • Improving access to care • Improving awareness regarding pediatric cancer • Developing adapted clinical research programs • Help local support
Teaching and training French-African Paediatric Oncology GroupGFAOP • Nurses • Training in French units (2001 – 2008) : 30 • South to South cooperation (Morocco) : 3 • French nurses teaching in African Units : 4 • Pathology lab. technicians • PCD courses (Yaounde) : 3 • French lab. (6 months stage) : 2
Teaching and training French-African Paediatric Oncology GroupGFAOP • Physicians • French National Diploma in PO(DIUOP) and 1 year hospital training • 8 GFAOP members attended and succeeded • Short 3 months training in Morocco • 1 physician • Workshops (1 to 3 ) at GFA meetings (1/year).
Therapeutic research • First study : 2001 – 2004 • Objective : Protocol feasibility in “African medical condition” • 2 protocols : Wilms tumor and Burkitt lymphoma • North Africa : almost unchanged SFCE or SIOP protocol • South to Sahara Units : ‘adapted’, less toxic • Second study : 2005 – 2008 • Objectives : • Improve the first results • Develop new protocols • 3 new protocols : • Cyclophosphamide in Burkitt lymphoma • Acute lymphoblastic leukemia • Hodgkin disease
Nephroblastoma First study : 2001 – 2004Second study : 2005 – 2008 Nephroblastoma GFAOP STUDIES
Clinical examination Abdominal US Chest RX • Localized stage • 4 x vincristine : 1,5 mg/m² • 2 x actino : 45 /kg • Metastatic stage • 6 x vincristine : 1.5 mg/m² • 3 x actino : 50 mg/m² Surgery + histology Staging Stage I : 2 courses 4 x vincristine : 1,5 mg/m² 2 x actinomycine D : 45 /kg Stage IV SIOP 2001 schedule good responders Surgery if needed Radiotherapy If necessary and available Stage II and III SIOP 2001 GFAOP-Nephro 2001 : Protocol strategy
Patients inclusion Nephroblastoma GFAOP STUDIES
80 Etude 2001-2004 70 Etude 2005-2008 60 50 40 30 20 10 0 Casa Alger Tana Tunis Dakar Rabat Ouaga Abidjan Bamako Yaoundé Patient Registration by Center Nephroblastoma GFAOP STUDIES
Stage Distribution • Based on surgical and/or pathological reports Study 1 Study 2 Nephroblastoma GFAOP STUDIES
Results : All population Nephroblastoma GFAOP STUDIES
Results : Comparison North Africa/ Sub Sahara units Nephroblastoma GFAOP STUDIES
Burkitt Lymphoma • 4 studies • Period I: LMB 89 modified protocols 2001-2004 • Burkitt-GFA 2001 • MAT(Morocco –Algeria –Tunisia) • Period II: 2005-2008 • Cyclo-Burkitt • MAT II(Morocco –Algeria – Tunisia) Burkitt lymphoma GFAOP STUDIES
Burkitt-GFAOP 2001 protocol Burkitt lymphoma GFAOP STUDIES
Burkitt lymphoma : 2001 – 2004 • 343 patients enrolled ; included 306 • Burkitt-GFAOP 2001 group : 187 • MAT group : 119 • Patients characteristics • Age : 1- 17 years (Med : 6y) • Sex ratio M/F : 1.9 • Tumors main locations • Abdominal : 242 • Facial : 131 Burkitt lymphoma GFAOP STUDIES
Burkitt lymphoma : 2001 – 2004 Burkitt lymphoma GFAOP STUDIES
OS according treatment regimen M.Harif Pediatr Blood Cancer 2008;50:1138–1142
Burkitt Lymphoma Second studies : 2005 – 2008 • North Africa : • MAT II protocol • Sub-Sahara units • Cyclo-Burkitt GFAOP protocol Burkitt lymphoma GFAOP STUDIES
N : 254 Burkitt lymphoma GFAOP STUDIES
Cyclo –Burkitt : Staging Burkitt lymphoma GFAOP STUDIES
Burkitt lymphoma GFAOP STUDIES
Burkitt lymphoma GFAOP STUDIES
Group A : 2 x COPAD Group B : COP 2 x COPADM 2 x CYM Group C : COP 2 x COPADM 2 x CYVE Seq 1, 2, 3, 4 MAT LMB 2005 protocol Burkitt lymphoma GFAOP STUDIES
MAT LMB 2005 : inclusion • 269 pts registered • 34 excluded • 235 included • 209 eligible Burkitt lymphoma GFAOP STUDIES
Patient Registration by Center Burkitt lymphoma GFAOP STUDIES
Other programs French-African Paediatric Oncology GroupGFAOP • Hodgkin • ALL • Retinoblastoma
HD – GFAOP : first analyzes • Units participating : 5 • Senegal, Madagascar, Mali, Cameroon, Ivory-Cost • Included : 30 • Patients characteristics • Age : 2 - 20 years (Med : 9y 9m) • Sex ratio M/F : 21/8 • Stages : • I/ II : 8 • III : 18 • IV : 4 • Evaluated : 14 • 12 CCR • 2 relapses
ALL - GFAOP protocol strategy Induction 5 weeks PRD DXM ; VCR ; L Aspa 2 IT Consolidation 12 weeks PRD ; VCR MTX ; 6 MP 3 IT Intensification 8 weeks DXM ; VCR Adria ; 6 MP ; Ara C 2 IT Maintenance 18 months 6 MP ; MTX 9 IT
ALL – GFAOP : first analyzes 4 Units : Cameroon, Madagascar Mali, Senegal • 50 patients enrolled • 38 confirmed and included • 32 eligible • 24 CR (80%) • 3 relapses • 8 deaths (4 early deaths)
Conclusion • Multicentric and prospecive studies feasible in Africa • Depending on the site : Easier in the North • Supportive care is improving • XRT missing in the South Results improving year after year
Groupe Franco-Africaind’Oncology Pediatric • Challenges • Tackling abandonment: Information, support for the families, improvement of access to care • Tackling diagnostic delay • Improving supportive care • Ethics • Data management • Expanding activity to other cancers, • Expanding activity to other regions and countries