Download
1 / 1
10 likes | 131 Views
Impact of the Immune Reconstitution Inflammatory Syndrome (IRIS) on Mortality and Hospitalization in HIV infected patients who started HAART in Mexico City J Hoyo-Ulloa I, Belaunzaran-Zamudio P, Crabtree-Ramirez B, Galindo-Fraga A, Pérez-Aguinaga M, Sierra-Madero J.

E N D
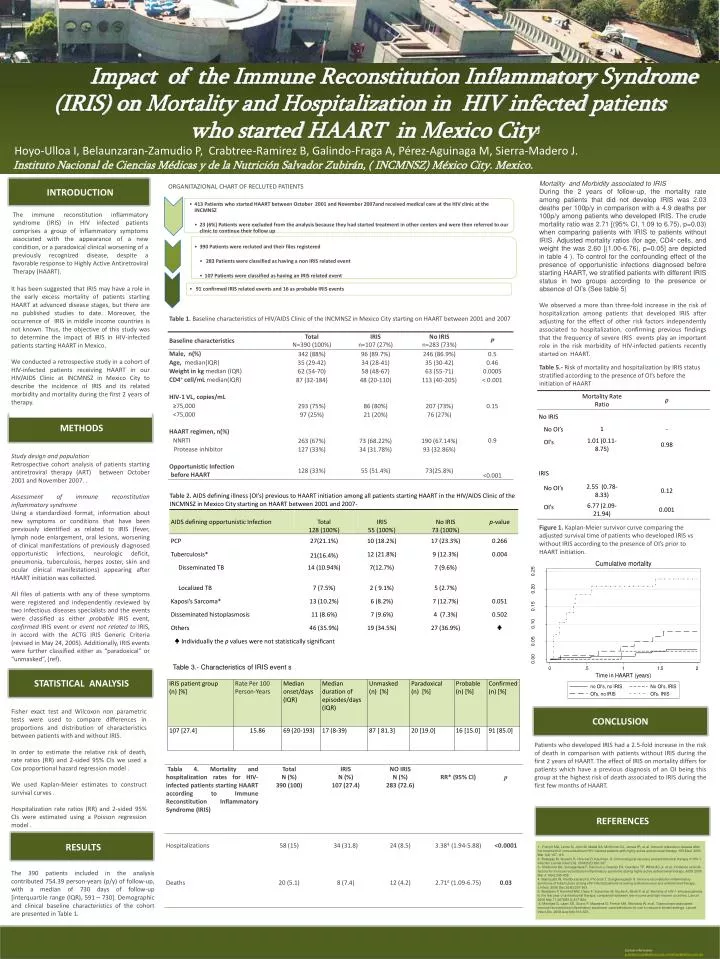
Impact of theImmuneReconstitutionInflammatorySyndrome (IRIS) onMortality and Hospitalization in HIV infectedpatients whostarted HAART in Mexico CityJ Hoyo-Ulloa I, Belaunzaran-Zamudio P, Crabtree-Ramirez B, Galindo-Fraga A, Pérez-Aguinaga M, Sierra-Madero J. Instituto Nacional de Ciencias Médicas y de la Nutrición Salvador Zubirán, ( INCMNSZ) México City. Mexico. INTRODUCTION Mortality and Morbidity associated to IRIS During the 2 years of follow-up, the mortality rate among patients that did not develop IRIS was 2.03 deaths per 100p/y in comparison with a 4.9 deaths per 100p/y among patients who developed IRIS. The crude mortality ratio was 2.71 [(95% CI, 1.09 to 6.75), p=0.03) when comparing patients with IRIS to patients without IRIS. Adjusted mortality ratios (for age, CD4+ cells, and weight the was 2.60 [(1.00-6.76), p=0.05] are depicted in table 4 ). To control for the confounding effect of the presence of opportunistic infections diagnosed before starting HAART, we stratified patients with different IRIS status in two groups according to the presence or absence of OI’s (See table 5) We observed a more than three-fold increase in the risk of hospitalization among patients that developed IRIS after adjusting for the effect of other risk factors independently associated to hospitalization, confirming previous findings that the frequency of severe IRIS events play an important role in the risk morbidity of HIV-infected patients recently started on HAART. ORGANITAZIONAL CHART OF RECLUTED PATIENTS The immune reconstitution inflammatory syndrome (IRIS) in HIV infected patients comprises a group of inflammatory symptoms associated with the appearance of a new condition, or a paradoxical clinical worsening of a previously recognized disease, despite a favorable response to Highly Active Antiretroviral Therapy (HAART). It has been suggested that IRIS may have a role in the early excess mortality of patients starting HAART at advanced disease stages, but there are no published studies to date. Moreover, the occurrence of IRIS in middle income countries is not known. Thus, the objective of this study was to determine the impact of IRIS in HIV-infected patients starting HAART in Mexico. We conducted a retrospective study in a cohort of HIV-infected patients receiving HAART in our HIV/AIDS Clinic at INCMNSZ in Mexico City to describe the incidence of IRIS and its related morbidity and mortality during the first 2 years of therapy. Table 5.- Risk of mortality and hospitalization by IRIS status stratified according to the presence of OI’s before the initiation of HAART METHODS Studydesign and population Retrospective cohort analysis of patients starting antiretroviral therapy (ART) between October 2001 and November 2007. . Assessment of immune reconstitution inflammatory syndrome Using a standardized format, information about new symptoms or conditions that have been previously identified as related to IRIS (fever, lymph node enlargement, oral lesions, worsening of clinical manifestations of previously diagnosed opportunistic infections, neurologic deficit, pneumonia, tuberculosis, herpes zoster, skin and ocular clinical manifestations) appearing after HAART initiation was collected. All files of patients with any of these symptoms were registered and independently reviewed by two infectious diseases specialists and the events were classified as either probable IRIS event, confirmed IRIS event or event not related to IRIS, in accord with the ACTG IRIS Generic Criteria (revised in May 24, 2005). Additionally, IRIS events were further classified either as “paradoxical” or “unmasked”, (ref). Table 2.AIDS defining illness (OI’s) previous to HAART initiation among all patients starting HAART in the HIV/AIDS Clinic of the INCMNSZ in Mexico City starting on HAART between 2001 and 2007- Figure 1. Kaplan-Meier survivor curve comparing the adjusted survival time of patients who developed IRIS vs without IRIS according to the presence of OI’s prior to HAART initiation. ♣Individually the p values were not statistically significant Table 3.- Characteristics of IRIS event s STATISTICAL ANALYSIS Fisher exact test and Wilcoxon non parametric tests were used to compare differences in proportions and distribution of characteristics between patients with and without IRIS. In order to estimate the relative risk of death, rate ratios (RR) and 2-sided 95% CIs we used a Cox proportional hazard regression model . We used Kaplan-Meier estimates to construct survival curves . Hospitalization rate ratios (RR) and 2-sided 95% CIs were estimated using a Poisson regression model . CONCLUSION . Patients who developed IRIS had a 2.5-fold increase in the risk of death in comparison with patients without IRIS during the first 2 years of HAART. The effect of IRIS on mortality differs for patients which have a previous diagnosis of an OI being this group at the highest risk of death associated to IRIS during the first few months of HAART. REFERENCES RESULTS 1.- French MA, Lenzo N, John M, Mallal SA, McKinnon EJ, James IR, et al. Immune restoration disease after the treatment of immunodeficient HIV-infected patients with highly active antiretroviral therapy. HIV.Med. 2000 Mar;1(2):107-115. 2.-Battegay M, Nuesch R, Hirschel B, Kaufman. G. Immunological recovery and antiretroviral therapy in HIV-1 infection Lancet.Infect.Dis. 2006;6(5):280-287. 3.-Shelburne SA, Visnegarwala F, Darcourt J, Graviss EA, Giordano TP, White AC,Jr, et al. Incidence and risk factors for immune reconstitution inflammatory syndrome during highly active antiretroviral therapy. AIDS 2005 Mar 4;19(4):399-406. 4.-Manosuthi W, Kiertiburanakul S, Phoorisri T, Sungkanuparph S. Immune reconstitution inflammatory syndrome of tuberculosis among HIV-infected patients receiving antituberculous and antiretroviral therapy. J.Infect. 2006 Dec;53(6):357-363. 5.-Braitstein P, Brinkhof MW, Dabis F, Schechter M, Boulle A, Miotti P, et al. Mortality of HIV-1-infected patients in the first year of antiretroviral therapy: comparison between low-income and high-income countries. Lancet 2006 Mar 11;367(9513):817-824. 6.-Meintjes G, Lawn SD, Scano F, Maartens G, French MA, Worodria W, et al. Tuberculosis-associated immune reconstitution inflammatory syndrome: case definitions for use in resource-limited settings. Lancet Infect.Dis. 2008 Aug;8(8):516-523. The 390 patients included in the analysis contributed 754.39 person-years (p/y) of follow-up, with a median of 730 days of follow-up [interquartile range (IQR), 591 – 730]. Demographic and clinical baseline characteristics of the cohort are presented in Table 1. REFERENCES *Contact information: Irma Hoyo MD E-mail: irmishoyo@yahoo.com.mx Contactinformation p_belaunzaran@yahoo.co.uk, irmishoyo@yahoo.com.mx






