Download
1 / 1
10 likes | 149 Views
Reference intervals and variations of total circulating matrix Gla protein (MGP) in healthy subjects. Silaghi N. Ciprian 1 , Gheorghe R. Simona 1 , Iovan V. Ciprian 2 , Crăciun M. Alexandra 1

E N D
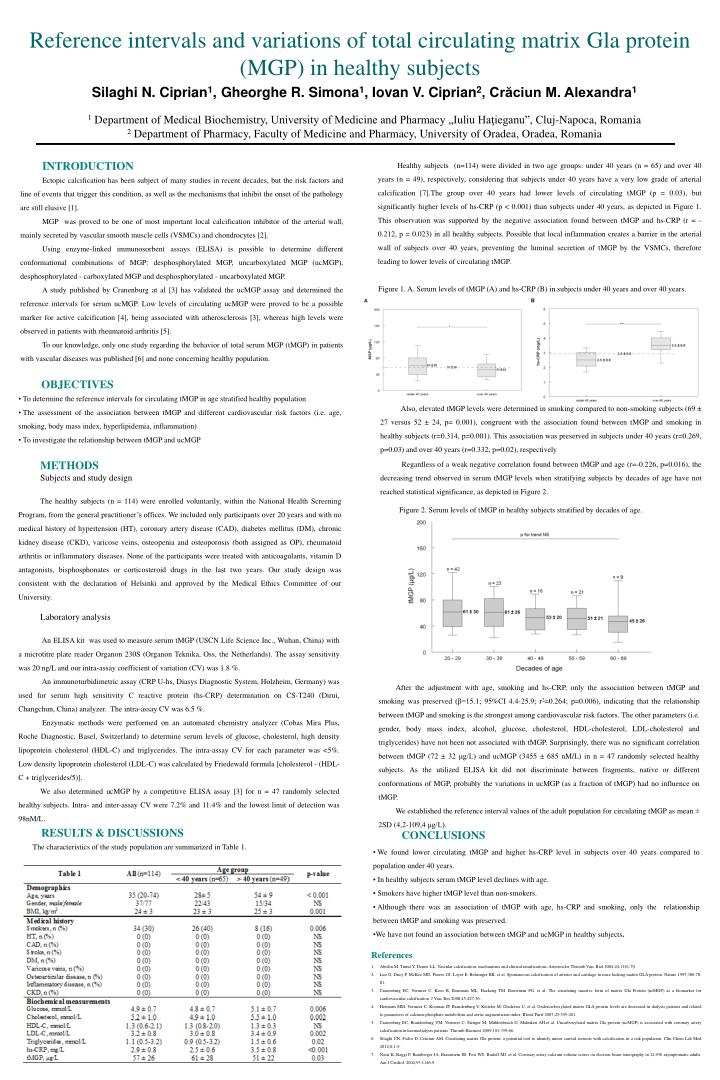
Reference intervals and variations of total circulating matrix Gla protein (MGP) in healthy subjects Silaghi N. Ciprian1,Gheorghe R. Simona1, Iovan V. Ciprian2, Crăciun M. Alexandra1 1 Department of MedicalBiochemistry, University of Medicine and Pharmacy „Iuliu Haţieganu”, Cluj-Napoca, Romania 2 Department of Pharmacy, Faculty of Medicine and Pharmacy, University of Oradea, Oradea, Romania INTRODUCTION Ectopic calcification has been subject of many studies in recent decades, but the risk factors and line of events that trigger this condition, as well as the mechanisms that inhibit the onset of the pathology are still elusive [1]. MGP was proved to be one of most important local calcification inhibitor of the arterial wall, mainly secreted by vascular smooth muscle cells (VSMCs) and chondrocytes [2]. Using enzyme-linked immunosorbent assays (ELISA) is possible to determine different conformational combinations of MGP: desphosphorylated MGP, uncarboxylated MGP (ucMGP), desphosphorylated - carboxylated MGP and desphosphorylated - uncarboxylated MGP. A study published by Cranenburg at al [3] has validated the ucMGP assay and determined the reference intervals for serum ucMGP. Low levels of circulating ucMGP were proved to be a possible marker for active calcification [4], being associated with atherosclerosis [3], whereas high levels were observed in patients with rheumatoid arthritis [5]. To our knowledge, only one study regarding the behavior of total serum MGP (tMGP) in patients with vascular diseases was published [6] and none concerning healthy population. Healthy subjects (n=114) were divided in two age groups: under 40 years (n = 65) and over 40 years (n = 49), respectively, considering that subjects under 40 years have a very low grade of arterial calcification [7].The group over 40 years had lower levels of circulating tMGP (p = 0.03), but significantly higher levels of hs-CRP (p < 0.001) than subjects under 40 years, as depicted in Figure 1. This observation was supported by the negative association found between tMGP and hs-CRP (r = - 0.212, p = 0.023) in all healthy subjects. Possible that local inflammation creates a barrier in the arterial wall of subjects over 40 years, preventing the luminal secretion of tMGP by the VSMCs, therefore leading to lower levels of circulating tMGP. Figure 1. A. Serum levels of tMGP (A) and hs-CRP (B) in subjects under 40 years and over 40 years. • OBJECTIVES • To determine the reference intervals for circulating tMGP in age stratified healthy population • The assessment of the association between tMGP and different cardiovascular risk factors (i.e. age, smoking, body mass index, hyperlipidemia, inflammation) • To investigate the relationship between tMGP and ucMGP Also, elevated tMGP levels were determined in smoking compared to non-smoking subjects (69 ± 27 versus 52 ± 24, p= 0.001), congruent with the association found between tMGP and smoking in healthy subjects (r=0.314, p=0.001). This association was preserved in subjects under 40 years (r=0.269, p=0.03) and over 40 years (r=0.332, p=0.02), respectively Regardless of a weak negative correlation found between tMGP and age (r=-0.226, p=0.016), the decreasing trend observed in serum tMGP levels when stratifying subjects by decades of age have not reached statistical significance, as depicted in Figure 2. METHODS Subjects and study design The healthy subjects (n = 114) were enrolled voluntarily, within the National Health Screening Program, from the general practitioner’s offices. We included only participants over 20 years and with no medical history of hypertension (HT), coronary artery disease (CAD), diabetes mellitus (DM), chronic kidney disease (CKD), varicose veins, osteopenia and osteoporosis (both assigned as OP), rheumatoid arthritis or inflammatory diseases. None of the participants were treated with anticoagulants, vitamin D antagonists, bisphosphonates or corticosteroid drugs in the last two years. Our study design was consistent with the declaration of Helsinki and approved by the Medical Ethics Committee of our University. Figure 2. Serum levels of tMGP in healthy subjects stratified by decades of age. Laboratory analysis An ELISA kit was used to measure serum tMGP (USCN Life Science Inc., Wuhan, China) with a microtitre plate reader Organon 230S (Organon Teknika, Oss, the Netherlands). The assay sensitivity was 20 ng/L and our intra-assay coefficient of variation (CV) was 1.8 %. An immunoturbidimetric assay (CRP U-hs, Diasys Diagnostic System, Holzheim, Germany) was used for serum high sensitivity C reactive protein (hs-CRP) determination on CS-T240 (Dirui, Changchun, China) analyzer. The intra-assay CV was 6.5 %. Enzymatic methods were performed on an automated chemistry analyzer (Cobas Mira Plus, Roche Diagnostic, Basel, Switzerland) to determine serum levels of glucose, cholesterol, high density lipoprotein cholesterol (HDL-C) and triglycerides. The intra-assay CV for each parameter was <5%. Low density lipoprotein cholesterol (LDL-C) was calculated by Friedewald formula [cholesterol - (HDL-C + triglycerides/5)]. We also determined ucMGP by a competitive ELISA assay [3] for n = 47 randomly selected healthy subjects. Intra- and inter-assay CV were 7.2% and 11.4% and the lowest limit of detection was 98nM/L. After the adjustment with age, smoking and hs-CRP, only the association between tMGP and smoking was preserved (β=15.1; 95%CI 4.4-25.9; r2=0.264; p=0.006), indicating that the relationship between tMGP and smoking is the strongest among cardiovascular risk factors. The other parameters (i.e. gender, body mass index, alcohol, glucose, cholesterol, HDL-cholesterol, LDL-cholesterol and triglycerides) have not been not associated with tMGP. Surprisingly, there was no significant correlation between tMGP (72 ± 32 μg/L) and ucMGP (3455 ± 685 nM/L) in n = 47 randomly selected healthy subjects. As the utilized ELISA kit did not discriminate between fragments, native or different conformations of MGP, probably the variations in ucMGP (as a fraction of tMGP) had no influence on tMGP. We established the reference interval values of the adult population for circulating tMGP as mean ± 2SD (4,2-109,4μg/L). • CONCLUSIONS • We found lower circulating tMGP and higher hs-CRP level in subjects over 40 years compared to population under 40 years. • In healthy subjectsserum tMGP level declines with age. • Smokers have higher tMGP level than non-smokers. • Although there was an association of tMGP with age, hs-CRP and smoking, only the relationship between tMGP and smoking was preserved. • We have not found an association between tMGP and ucMGP in healthy subjects. RESULTS & DISCUSSIONS The characteristics of the study population are summarized in Table 1. • References • Abedin M, Tintut Y, Demer LL. Vascular calcification: mechanisms and clinical ramifications. Arterioscler Thromb Vasc Biol 2004;24:1161-70. • Luo G, Ducy P, McKee MD, Pinero GJ, Loyer E, Behringer RR, et al. Spontaneous calcification of arteries and cartilage in mice lacking matrix GLA protein. Nature 1997;386:78-81. • Cranenburg EC, Vermeer C, Koos R, Boumans ML, Hackeng TM, Bouwman FG, et al. The circulating inactive form of matrix Gla Protein (ucMGP) as a biomarker for cardiovascular calcification. J Vasc Res 2008;45:427-36. • Hermans MM, Vermeer C, Kooman JP, Brandenburg V, Ketteler M, Gladziwa U, et al. Undercarboxylated matrix GLA protein levels are decreased in dialysis patients and related to parameters of calcium-phosphate metabolism and aortic augmentation index. Blood Purif 2007;25:395-401. • Cranenburg EC, Brandenburg VM, Vermeer C, Stenger M, Mühlenbruch G, Mahnken AH,et al. Uncarboxylated matrix Gla protein (ucMGP) is associated with coronary artery calcification in haemodialysis patients. Thromb Haemost 2009;101:359-66. • Silaghi CN, Fodor D, Crăciun AM. Circulating matrix Gla protein: a potential tool to identify minor carotid stenosis with calcification in a risk population. Clin Chem Lab Med 2012;0:1-9. • Nasir K, Raggi P, Rumberger JA, Braunstein JB, Post WS, Budoff MJ, et al. Coronary artery calcium volume scores on electron beam tomography in 12,936 asymptomatic adults. Am J Cardiol. 2004;93:1146-9.