Download
1 / 29
320 likes | 1.04k Views
Pectus excavatum (PE). There is a large group of congenital abnormalities of the thoracic cage that manifest as deformities of the anterior chest wall. Question: How many groups of the deformities of the anterior chest wall ?. Answer This diverse group includes : pectus excavatum

E N D
There is a large group of congenital abnormalities of the thoracic cage that manifest as deformities of the anterior chest wall.
Question: How many groups of the deformities of the anterior chest wall ?
Answer This diverse group includes : • pectus excavatum • pectus carinatum • Pouter pigeon breast • poland syndrome • cleft sternum
Pectus excavatum (PE) is the most common chest wall malformation and one of the most frequent major congenital anomalies. • It approximately occurs in 1 in every 400 births, with a 4:1 male predominance.
In patients with PE, the sternum and adjacent chest wall are displaced posteriorly toward the spine, creating a depression of the anterior chest wall.
A preoperative computed tomography (CT) chest scan is currently recommended by some authors to evaluate the extent of the deformity and to plan repair.
Pathogenesis • The currently acceptedetiologic theory is thatexcessive growth of the lower costalb cartilages (gristle)occursthat forcesthe sternum into a concave position. • The reason for this overgrowth of costal cartilages, which frequently increases the severity of the deformity in the preschool-age child andagain during the pubertal years, is currentlyunknown.
Symptoms • Symptoms are infrequent during early childhood, apart from a shy awareness of the abnormality and a typical unwillingness to expose the chest while swimming or taking part in other social or athletic activities.
It is particularly important that this deformity be corrected, if possible, before the child starts school,because it may cause severe psychologica(mental) and emotional damage.
During early adolescence • Easy fatigability • Shortness of breath with mild exercise • Decreased stamina • Tachycardia(bradycardia),and/or palpitations are common • Pectus excavatum patients commonly try hard to keep up with their peers physically
Treatment • Resect a major portion of the deformed costal cartilages。 • The sternal osteotomy and resection of short segments of cartilages from the deformed ribs.
A new minimally invasive(invade) technique for repair of PE (MIRPE) was reported by Nuss et al. in 1998 for young children (mean age under 5 years)
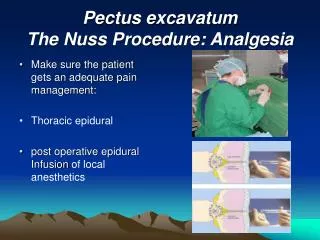
Minimally invasive repair using a convex steel bar guided across the chest through a substernal tunnel and then twisted with a wrench to force the convex side anteriorly, which elevates the depressed sternum and deformed costal cartilages. The Nuss procedure
Recent modifications of the MIRPE adopted by many surgeons include the use of thoracoscopy to visualize passage of the clamp behind the sternum
References • Feng J, Hu T, Liu W, Zhang S, Tang Y, Chen R, Jiang X, Wei F:The biomechanical, morphologic, and histochemical properties of the costal cartilages in children with pectus excavatum.J Pediatr Surg 2001,36(12):1770-1776 • Fokin AA, Steuerwald NM, Ahrens WA, Allen KE:Anatomical, histologic,and genetic characteristics of congenital chest wall deformities.Semin Thorac Cardiovasc Surg2009,21(1):44-57. • Hebra A. Minimally invasive pectus surgery. Chest Surg. Clin. N. Am.2000;10:329–339 • Molik KA, Engum SA, Rescorla FJ, et al. Pectus excavatum repair:experience with standard and minimal invasive techniques. J. Pediatr.Surg. 2001;36:324–328 • Nuss D, Kelly RE Jr, Croitoru DP, et al. A ten-year review of a mini-mally invasive technique for the correction of pectus excavatum. J. Pe-diatr. Surg. 1998;33:545–552 • Eric W. Fonkalsrud, M.D. Current Management of Pectus Excavatum. World J. Surg. 27, 502–508, 2003 • Martinez D, Juame J, Stein T, et al. The effect of costal cartilage resection on chest wall development. Pediatr. Surg. Int. 1990;5:170–173