Download
1 / 64
730 likes | 1.17k Views
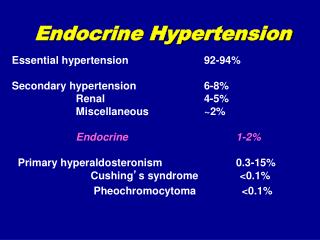
Hypertension associated with Endocrine Disorders. Hypertension assoc with Endocrine Disorders Background. Prevalence/Incidence- Unknown Requires the application of highly sensitive and specific screening tests Expensive and not risk free Clues helpful in identifying patients

E N D
Hypertension assoc with Endocrine DisordersBackground • Prevalence/Incidence- Unknown • Requires the application of highly sensitive and specific screening tests • Expensive and not risk free • Clues helpful in identifying patients • Hypertension at a young age • Essential hypertension onset typically 40s+ • Sudden onset or increased severity • Drug resistant hypertension
Hypertension assoc with Endocrine DisordersBackground • Most common forms • Primary aldosteronism • Pheochromocytoma • Cushings
Primary AldosteronismPrevalence and Pathophysiology • Second only to renal vascular hypertension as a cause of curable hypertension • 2 large studies in known hypertensives revealed a prevalence exceeding 9%
Primary AldosteronismPrevalence and Pathophysiology Insert a picture of renal distal tubule and exchange of K and H for Na -hypervolemia/hypertension 2nd to increased Na -alkalosis 2nd to decreased H+ and decreased K+
Primary AldosteronismPrevalence and Pathophysiology • Associated findings • Hypernatremia • Usually in the range of 143-147 • Hypervolemia • Usually without peripheral edema– due to aldosterone escape (probably mediated by atrial naturitic peptide and a pressure naturesis). Confirmed by decreased renin levels. • Hypertension • Due to the mild volume expansion (as above)
Primary AldosteronismPrevalence and Pathophysiology Hypokalemia • Esp intracellular depletion, leading to glucose intolerance, EKG changes c/w LVH, muscle weakness, and polyuria • Must have adequate sodium delivery for this to occur • If sodium restricted, no hypertension/no hypokalemia • If volume depleted (less distal sodium delivery), also no hypokalemia • That is why diuretics (HCTZ) paradoxically improves K levels • Hypomagnesemia • Renal cysts- 2nd to hypokalemia
Primary AldosteronismScreening tests • Serum potassium level • Traditionally advocated as the most effective single screening test • One large study revealed normal plasma K levels in ALL patients with primary aldosteronism (Fardella, J Clin Endo Meta 2000) • Another study (Loh, JCEM) only 6/16 with biochemically confirmed hyperaldo had hypokalemia • 20% of surgically confirmed hyperaldo have normal plasma K • Some argue serum K artificially high due to increased hemolysis which is increased in hyperaldosterone states
Primary AldosteronismScreening tests • Serum potassium level • Traditionally advocated as the most effective single screening test • GRH usually doesn’t have hypokalemia • But the aldo in this disease is under ACTH stimulation which peaks in the am. Therefore only exposed to elevated levels for transient periods • So recommended to w/u for hyperaldo, even with a normal K, if: • Severe or refractory hypertension • Onset at a young age • Sudden increase in BP
Primary AldosteronismScreening tests • Serum potassium level • If it is truly low, then measure a 24hr urine potassium • If >30meq/day in the face of hypokalemia, then renal wasting (hyperaldo) is present • If <30meq/day, the hypokalemia is due to an extrarenal source • Vomiting • Diarrhea • As K excretion is dependent upon adequate distal sodium delivery • Patient should be on a normal to high Na diet (so check a concurrent urine Na) • Can be used as a screening test as well– if increased Na decreases K, this is a strong indication of non-suppressible aldosteronism
Primary AldosteronismScreening tests • Low renin • Better screening test • Almost all cases of uncomplicated primary aldosteronism have low renin. Suppressed by: • Elevated blood pressure • Elevated sodium and expanded extracellular volume
Primary AldosteronismScreening tests • Low renin • Not diagnostic of hyperaldo • 40% of patients with essential hypertension manifest suppressed plasma renin levels • Anti-hypertensive agents also known to lower renin levels • Antisympathetic drugs, central or peripheral can suppress plasma renin levels (How?) • Beta-blockers also suppress plasma renin levels
Primary AldosteronismScreening tests • Aldo/PRA level—any provocative measures? • Most sensitive and specific screening test • Performed only after agents known to suppress renin (beta-blockers and alpha-blockers) have been discontinued- no consensus on with or without medications • Draw out the feedback mechanism • > 30 = primary aldosteronism, usually a unilateral adenoma • 15-30 = suggestive of aldosteronism, usually due to bilateral adrenal hyperplasia
Primary AldosteronismScreening tests • Aldo/PRA level—any provocative measures? • Best to try and suppress aldo and stimulate pra • Suppress aldo– avoid K loading and maximize the volume status (250meq Na qd x 3 days with liberal water intake). Recumbent • Stimulate PRA- standing or hypovolemic (diuretics) • As can see, if you stimulate one, you suppress the other • If you suppress aldo, you suppress renin, so ratio doesn’t change • If you stimulate PRA, you stimulate aldo- so ratio doesn’t change
Primary AldosteronismScreening tests • Aldo/PRA level • Theoretically can even be used with drugs known to stimulate renin release • Including: diuretics, ACE inhibitors, calcium channel blockers, and other vasodilators • Might decrease sensitivity slightly • A positive test would still be valid • A negative test might not be definitive, because the increased renin level might artificially lower the ratio • Best to try on the drugs first- it can allow you to safely make the diagnosis without withdrawing the drugs
Primary AldosteronismDiagnosis • Traditionally • Demonstration of excessive aldosterone production plus suppression of the normal stimulus (renin/angio II) • Required suppressive maneuvers to demonstrate hyperaldo • Several days of high salt diet, intramuscular mineralocorticoids to ensure sodium retention and volume expansion, or bolus of NS • Required a stimulative maneuvers to demonstrate suppressed renin levels • Low salt diet + diuretic
Primary AldosteronismDiagnosis • Currently • Application of the standard screening test– unstimulated aldo/pra level in a patient not taking any drugs known to impact the axis (which leaves what?) • Drug effect • What about K level– • If high– stimulates aldo • If low– suppress aldo • Must it be in the normal range for these tests? • I would think low is ok, but high must be treated
Primary AldosteronismDifferentiation of Subtypes • Unilateral adrenal adenoma • Most common form of primary aldosteronism • 60-65% of the cases • Most amenable to surgical intervention • Usually small (1 cm or less) • Therefore localization techniques based on anatomy alone may not be effective • MRI- only 60% sensitive • Adrenal venography- dangerous • Isotopoic scanning- disappointing
Primary AldosteronismDifferentiation of Subtypes • Unilateral adrenal adenoma • Biochemical techniques the best • Unilateral adenoma is modulated by ACTH, but not angiotensin II • Why? • Adenoma is closer to malignancy, therefore more autonomous and less likely to respond to normal feed back. Versus hyperplasia which is still responsive to normal feedback, just at an elevated level
Primary AldosteronismDifferentiation of Subtypes • Unilateral adenoma is modulated by ACTH, but not angiotensin II • Check aldo level when renin system quiescent (early morning after sleeping recumbent) but ACTH maximally stimulated by morning surge • Check aldo again after activation of the renin system- in the afternoon or after a diuretic dose, when the ACTH system is quiescent • Unilateral– high aldo in am (with ACTH surge) and lower in the pm (refractory to renin surge) • Bilateral- lower in the am due to quiescent renin system, then peaking in the pm with the increased renin
Primary AldosteronismDifferentiation of Subtypes • Unilateral adenoma is modulated by ACTH, but not angiotensin II • Check aldo level when renin system quiescent (early morning after sleeping recumbent) but ACTH maximally stimulated by morning surge • Check aldo again after activation of the renin system- in the afternoon or after a diuretic dose, when the ACTH system is quiescent • Unilateral– high aldo in am (with ACTH surge) and lower in the pm (refractory to renin surge) • Bilateral- lower in the am due to quiescent renin system, then peaking in the pm with the increased renin
Primary AldosteronismDifferentiation of Subtypes • Adrenal venous blood sampling • Most sensitive and specific way of separating unilateral and bilateral forms of the disorder • Test often misleading due to errors • Right adrenal vein difficult to locate • Multiple adrenal venous drainage or adrenal effluent diluted by blood from other sources such as the phrenic vein or left renal vein
Primary AldosteronismDifferentiation of Subtypes • Attempts made to minimize these errors by giving a continuous infusion of ACTH (which stimulates cortisol) during the sampling • By expressing sampling as ratio of aldosterone to cortisol • Correct for dilution of the adrenal venous blood • Even allows for identification in the absence of the ability to sample on adrenal vein • Check the ratio in the IVC, if higher, then the lesion is in the unsampled gland
Primary AldosteronismTreatment • Unilateral lesion • Adrenalectomy almost always uniformly effective in eliminating the hyperaldosteronism • 70% of people can be withdrawn for anti-hypertensive agents completely • May take months before the final nadir in blood pressure is seen
Primary AldosteronismTreatment • Bilateral disease • Medical treatment is preferred • Traditionally, spironolactone is the agent of choice • Required high dose– up to 800mg/day • Painful gynecomastia, impotence, and decreased libido often leads to discontinuation. Women also affected- menstrual irregularities • Amiloride is my drug of choice • 5 mg po bid, increased to 15mg po bid • Same effect as spironolactone with rare side effects • Usually requires HCTZ as adjunct
Primary AldosteronismTreatment • Bilateral disease • ACE-I are still effective • Would expect a poor response given the relatively low renin/angio II state • However patients with bilateral disease may simply be due to increased sensitivity to even low levels of angio II– therefore blocking it is very effective
PheochromocytomaBackground • Less frequent than primary aldosteronism • First manifestation can be a catastrophic outcome • Must r/o in a hypertensive pregnant patient with labile bp • Symptoms are protean • Usually directly attributable to catacholeamine excess and thus must be differentiated from other syndromes of catecholamine excess (also known as pseudopheochromocytoma) • Only 1 in 300 work-ups positive
PheochromocytomaBackground • 85% result from adrenal medullary tumors • If extra adrenal, almost always below the diaphragm (usually in the periaortic area) • Can be associated with MEN syndromes • IIa- assoc with thyroid and parathyroid tumors • IIb- assoc ganglioneuromas- Von Hippel-Lindau syndrome and other neuroectodermal abnormalities
PheochromocytomaSymptoms • Non-specific • Headache, diaphoresis, pallor, tachycardia, anxiety or tremulousness, nausea, weakness, chest pain, dyspnea, fever, weight loss • Sustained elevation of bp is the most frequent finding • But 1/3 patients have episodic or paroxysmal hypertension • 10-15% have normal blood pressure • In a recent Italian review of 284 pts, • 67% paroxysmal, 59% hypertensive crisis, and 21% normal bp
PheochromocytomaSymptoms • Non-specific • Grade III or IV hypertensive retinopathy • In >50% of patients • Presumably owing to the intense vasoconstriction resulting from the excessive catecholamine production • Dilated cardiomyopathy- due to the toxic effects of long term catechols • Secondary erythrocytosis due to overproduction of erythropoietin
PheochromocytomaSymptoms • Paroxysmal nature of symptoms • Understandable given the variety of stimuli of catecholamine release, with an exaggerated response occurring in pheochromocytoma cases
PheochromocytomaBackground • Normotensive or hypotensive variants • Suggested that the intense vasoconstriction and elevated bp induced by the release of catecholamines • Result in a contracted intravascular volume (like a cold induced diuresis) • Suppressed baroreceptor reflex • Also could be the result of release of “renal-dose dopamine” by the tumor • Resulting in generalized vasodilitation
PheochromocytomaBackground • Paradoxical rise in BP with anti-hypertensive medications • Beta-blockers can cause a paradoxical hypertension • Due to the resulting unopposed alpha induced vasoconstriction
PheochromocytomaBackground • Metabolic abnormalities • Hyperglycemia and glucose intolerance • Associated with epinephrine induced insulin resistance • Lipid abnormalities • Hypokalemia • Due to cellular shifts associated with epi release
PheochromocytomaPseudo-pheochromocytoma • Pheo mimicked by a variety of circumstances • All usually feature excessive catecholamine production or stimulation of adrenergic receptors • Use of sympathomimetic agents- nasal sprays, cold remedies, diet aids, ephedrine, amphetamines, • Administration of drugs with containing sympathomimetic side effects- imipramine and amitrypiptyline (esp if given MAO-Is*) • Addictive Substance withdrawal • Withdrawal from alpha or beta-blockers
PheochromocytomaPseudo-pheochromocytoma • MAO-Is • 3 currently available in the United States • All three are anti-depressant drugs • Nardil (phenelzine) • Parnate (tranylcypromine) • Marplan (isocarboxazid)
PheochromocytomaPseudo-pheochromocytoma • Pheo mimicked by a variety of circumstances • All usually feature excessive catecholamine production or stimulation of adrenergic receptors • Use of sympathomimetic agents- nasal sprays, cold remedies, diet aids, ephedrine, amphetamines, • Administration of drugs with containing sympathomimetic side effects- imipramine and amitrypiptyline (esp if given MAO-Is) • Addictive Substance withdrawal • Withdrawal from alpha or beta-blockers
PheochromocytomaScreening Tests • Availability of sensitive and specific measures of catechols and their metabolites in urine and plasma, provides for safer, convenient, and reasonably accurate was to screen. • Still fraught with inaccuracy • Plasma values for catechols can be in the normal range if the tumor releases catechols intermittently • Urine studies can be incomplete collections. Spot samples can be in error if episodic hormone release • Choice of specific metabolite for measurement • Often required to check total catechols, norepi, metanephrine, normetanephrine, vanillylmandelic acid, and/or homovanillic acid to ensure the patient does not have a pheo
PheochromocytomaScreening Tests • Most antihypertensive agents elevate catechols • Exceptions- centrally acting alpha-adrenergic agonists (clonidine, guanabenz, guanfacine) and reserpine) • Much like with hyperaldo • First do the screening tests while on their baseline medications • Then if elevated, you are forced to change their anti-hypertensive regimen to r/o a drug induced false-positive
PheochromocytomaScreening Tests • Measurement of plasma or urine catecholamines and metabolites is diagnostic in 95% of patients with symptoms • Uncertainty regarding the “best” test • Urinary catecholamine • Nearly all patients will have an elevated value for catechols and metabolites • Larger tumors have more metabolites (VMA and Metanephrines) due to metabolism within the tumor itself • Smaller tumors have a greater proportion of free catechols • Urinary total metanephrines • May be the most useful test • Lest likely to be affected by drugs and foods ***** • Above 1.2 mg/day is highly suggestive of pheo • False positive occurs with buspirone (metabolite measured as a metanephrine)
PheochromocytomaScreening Tests • Measurement of plasma or urine catecholamines and metabolites is diagnostic in 95% of patients with symptoms • Uncertainty regarding the “best” test • Plasma catecholamines • Total catechol level (Norepi + epi) • >2000 pg/mL in a supine patient with an indwelling cath x 30 minutes is diagnostic • >950 pg/mL is suggestive • Because false positives are common, should also combine with suppression testing • Give 0.3mg of clonidine • Measure total catechols before and 3 hours after -No pheo, the level will drop to <500
PheoDiagnosis • Localization • Most pheos are > 2cm in diameter • CT sensitivity- 99% for intraadrenal and 91% for extra adrenal tumors • MIBG isotopic scan- slightly lower sensitivity at 88.5% • Because hemorrhagic necrosis and subsequent calcification are frequent • Often seen on plain films
PheochromocytomaTreatment • Preferred treatment is surgical removal of the tumor • Surgeon must ligate the major blood supplies to reduce the amount of catechols introduced into circulation • 7-10 days of pre-operative alpha-adrenergic blockade prior to surgery • Not for bp or arrhythmia control intra-op • To permit the contracted intravascular volume to return to normal • Otherwise the vasodilitation associated with tumor removal results in profound hypotension
PheochromocytomaFollow-up • Multiple and malignant tumors occur in about 10% of patients • Requires q 6-12 month follow-up • Don’t forget to screen family members • Need to r/o a familial (MEN-type) syndrome • Esp if tumor is epi predominant
Pheochromocytoma“Think of it, confirm it, find it, and remove it” • Think of it • Mayo review of over 40,000 autopsies found 54 pheos, • 41 (76% ) not diagnosed until the time of death • 23 (55%) had retrospectively been the cause of death • Swedish study (Svardsudd) found similar results • 40% had the diagnosis made at autopsy
Pheochromocytoma“Think of it, confirm it, find it, and remove it” • Think of it • NE tumors • Primarily present with stable hypertension • Just like being on a chronic norepi drip • Epi tumors • Primarily associated with adrenaline-like symptoms • Can have hypoK, hyperglycemia
Pheochromocytoma“Think of it, confirm it, find it, and remove it” • Think of it • Differential diagnosis
Pheochromocytoma“Think of it, confirm it, find it, and remove it” • Confirm it • Typically requires biochemical diagnosis • Don’t go looking with a CT first • Rate of incidentalomas = XXXX • If you clinically suspect a pheo and get a scan first, it will be nearly impossible to r/o an incidentalomas. You have just committed the patient to surgery
PheochromocytomaBiochemical Diagnosis • Diagnosis requires evidence of excessive catecholamine production by the tumor • Usually achieved by measurement of catechols and metabolites in urine or plasma • Unfortunately, norepi and epi are also produced by sympathetic nerves and the adrenal medulla, and therefore not specific for pheochromocytoma • High levels of catechols and metabolites can be produced disease states associated with increased sympathetic nervous and adrenal medullary release
PheochromocytomaBiochemical Diagnosis • Understanding catecholamine release and metabolism under normal conditions as well as disease states, can help understanding the utility and limitations of biochemical tests for the diagnosis of pheochromocytoma