Download
1 / 1
10 likes | 26 Views
This study estimates the burden of rotavirus gastroenteritis among children in the Middle East and North Africa, including mortality rates, genotype distribution, and healthcare resource utilization and costs.

E N D
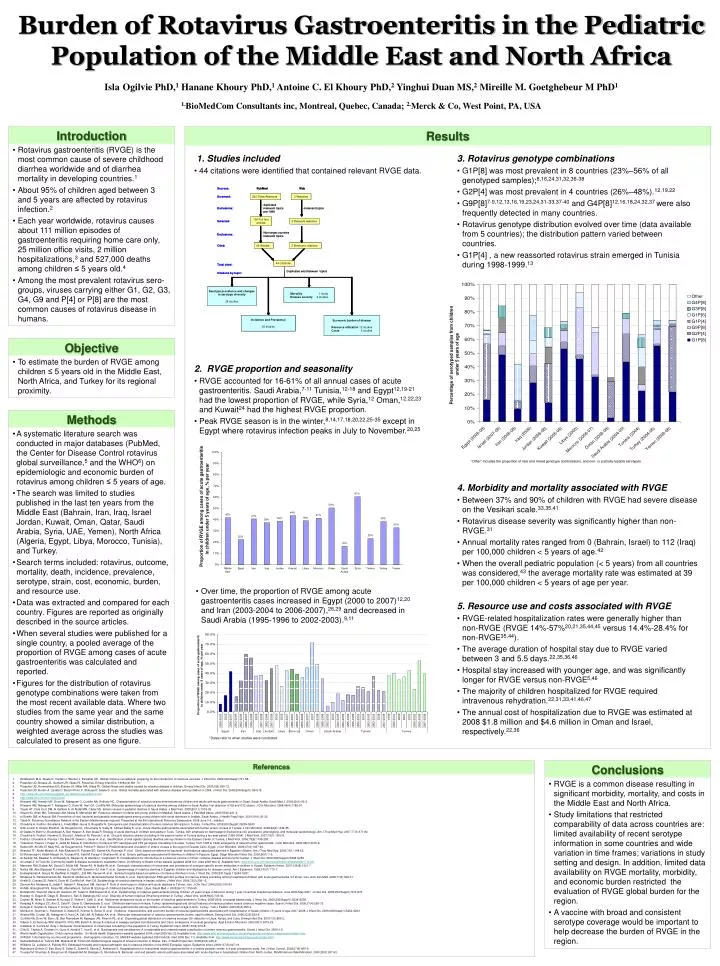
Introduction • Rotavirus gastroenteritis (RVGE) is the most common cause of severe childhood diarrhea worldwide and of diarrhea mortality in developing countries.1 • About 95% of children aged between 3 and 5 years are affected by rotavirus infection.2 • Each year worldwide, rotavirus causes about 111 million episodes of gastroenteritis requiring home care only, 25 million office visits, 2 million hospitalizations,3 and 527,000 deaths among children ≤ 5 years old.4 • Among the most prevalent rotavirus sero-groups, viruses carrying either G1, G2, G3, G4, G9 and P[4] or P[8] are the most common causes of rotavirus disease in humans. • Objective • To estimate the burden of RVGE among children ≤ 5 years old in the Middle East, North Africa, and Turkey for its regional proximity. • Methods • A systematic literature search was conducted in major databases (PubMed, the Center for Disease Control rotavirus global surveillance,5 and the WHO6) on epidemiologic and economic burden of rotavirus among children ≤ 5 years of age. • The search was limited to studies published in the last ten years from the Middle East (Bahrain, Iran, Iraq, Israel Jordan, Kuwait, Oman, Qatar, Saudi Arabia, Syria, UAE, Yemen), North Africa (Algeria, Egypt, Libya, Morocco, Tunisia), and Turkey. • Search terms included: rotavirus, outcome, mortality, death, incidence, prevalence, serotype, strain, cost, economic, burden, and resource use. • Data was extracted and compared for each country. Figures are reported as originally described in the source articles. • When several studies were published for a single country, a pooled average of the proportion of RVGE among cases of acute gastroenteritis was calculated and reported. • Figures for the distribution of rotavirus genotype combinations were taken from the most recent available data. Where two studies from the same year and the same country showed a similar distribution, a weighted average across the studies was calculated to present as one figure. Burden of Rotavirus Gastroenteritis in the Pediatric Population of the Middle East and North AfricaIslaOgilvie PhD,1 Hanane Khoury PhD,1 Antoine C. El Khoury PhD,2 Yinghui Duan MS,2 Mireille M. Goetghebeur M PhD11.BioMedCom Consultants inc, Montreal, Quebec, Canada; 2.Merck & Co, West Point, PA, USA Results • 1. Studies included • 44 citations were identified that contained relevant RVGE data. • 3. Rotavirus genotype combinations • G1P[8] was most prevalent in 8 countries (23%–56% of all genotyped samples);8,16,24,31,32,36-38 • G2P[4] was most prevalent in 4 countries (26%–48%).12,19,22 • G9P[8]7-9,12,13,16,19,23,24,31-33,37-40 and G4P[8]12,16,18,24,32,37 were also frequently detected in many countries. • Rotavirus genotype distribution evolved over time (data available from 5 countries); the distribution pattern varied between countries. • G1P[4] , a new reassorted rotavirus strain emerged in Tunisia during 1998-1999.13 • 2. RVGE proportion and seasonality • RVGE accounted for 16-61% of all annual cases of acute gastroenteritis. Saudi Arabia,7-11 Tunisia,12-18 and Egypt12,19-21 had the lowest proportion of RVGE, while Syria,12 Oman,12,22,23 and Kuwait24 had the highest RVGE proportion. • Peak RVGE season is in the winter,8,14,17,18,20,22,25-35 except in Egypt where rotavirus infection peaks in July to November.20,25 “Other” includes the proportion of rare and mixed genotype combinations, and non- or partially-typable serotypes • 4. Morbidity and mortality associated with RVGE • Between 37% and 90% of children with RVGE had severe disease on the Vesikari scale.33,35,41 • Rotavirus disease severity was significantly higher than non-RVGE.31 • Annual mortality rates ranged from 0 (Bahrain, Israel) to 112 (Iraq) per 100,000 children < 5 years of age.42 • When the overall pediatric population (< 5 years) from all countries was considered,43 the average mortality rate was estimated at 39 per 100,000 children < 5 years of age per year. • Over time, the proportion of RVGE among acute gastroenteritis cases increased in Egypt (2000 to 2007)12,20 and Iran (2003-2004 to 2006-2007),26,29 and decreased in Saudi Arabia (1995-1996 to 2002-2003).9,11 • 5. Resource use and costs associated with RVGE • RVGE-related hospitalization rates were generally higher than non-RVGE (RVGE 14%-57%20,21,35,44,45 versus 14.4%-28.4% for non-RVGE35,44). • The average duration of hospital stay due to RVGE varied between 3 and 5.5 days.22,35,36,46 • Hospital stay increased with younger age, and was significantly longer for RVGE versus non-RVGE5,46 • The majority of children hospitalized for RVGE required intravenous rehydration.22,31,33,41,46,47 • The annual cost of hospitalization due to RVGE was estimated at 2008 $1.8 million and $4.6 million in Oman and Israel, respectively.22,36 *Dates refer to when studies were conducted • References • Widdowson M-A, Steele D, Vojdani J, Wecker J, Parashar UD. Global rotavirus surveillance: preparing for the introduction of rotavirus vaccines. J Infect Dis. 2009;200(Suppl1):S1-S8. • Parashar UD, Bresee JS, Gentsch JR, Glass RI. Rotavirus. Emerg Infect Dis. 1998;4(4):561-70. • Parashar UD, Hummelman EG, Bresee JS, Miller MA, Glass RI. Global illness and deaths caused by rotavirus disease in children. Emerg Infect Dis. 2003;9(5):565-72. • Parashar UD, Burton A, Lanata C, Boschi-Pinto C, Shibuya K, Steele D, et al. Global mortality associated with rotavirus disease among children in 2004. J Infect Dis. 2009;200(Suppl1):S9-S15. • http://www.cdc.gov/rotavirus/global_surveillance/surveillance.htm • http://www.who.int/nuvi/rotavirus/en • Kheyami AM, Areeshi MY, Dove W, Nakagomi O, Cunliffe NA, Anthony HC. Characterization of rotavirus strains detected among children and adults with acute gastroenteritis in Gizan, Saudi Arabia. Saudi Med J. 2008;29(1):90-3. • Kheyami AM, Nakagomi T, Nakagomi O, Dove W, Hart CA, Cunliffe NA. Molecular epidemiology of rotavirus diarrhea among children in Saudi Arabia: first detection of G9 and G12 strains. J Clin Microbiol. 2008;46(4):1185-91. • Tayeb HT, Dela Cruz DM, Al Qahtani A, Al Ahdal MN, Carter MJ. Enteric viruses in pediatric diarrhea in Saudi Arabia. J Med Virol. 2008;80(11):1919-29. • Ghazi HO, Khan MA, Telmesani AM, Idress B, Mahomed MF. Rotavirus infection in infants and young children in Makkah, Saudi Arabia. J Pak Med Assoc. 2005;55(6):231-4. • el Sheikh SM, el Assouli SM. Prevalence of viral, bacterial and parasitic enteropathogens among young children with acute diarrhoea in Jeddah, Saudi Arabia. J Health Popul Nutr. 2001;19(1):25-30. • Teleb N. Rotavirus Surveillance Network in the Eastern Mediterranean regional. Presented at the 8th International Rotavirus Symposium; 2008 June 3-4.; Istanbul. • Chouikha A, Fodha I, Bouslama L, Fredj MBH, Jaoua S, Boujaafar N. Emergence and characterization of human rotavirus G9 strains in Tunisia. J Infect Dis. 2009;200(Suppl1):S239-S243. • Sdiri-Loulizi K, Gharbi-Khelifi H, de Rougemont A, Chouchane S, Sakly N, Ambert-Balay K, et al. Acute infantile gastroenteritis associated with human enteric viruses in Tunisia. J Clin Microbiol. 2008;46(4):1349-55. • Al Gallas N, Bahri O, Bouratbeen A, Ben Haasen A, Ben Aissa R. Etiology of acute diarrhea in children and adults in Tunis, Tunisia, with emphasis on diarrheagenic Escherichia coli: prevalence, phenotyping, and molecular epidemiology. Am J Trop Med Hyg. 2007;77(3):571-82. • Chouikha A, Fodha I, Noomen S, Bouzid L, Mastouri M, Peenze I, et al. Group A rotavirus strains circulating in the eastern center of Tunisia during a ten-year period (1995-2004). J Med Virol. 2007;79(7):1002-8. • Fodha I, Chouikha A, Peenze I, De Beer M, Dewar J, Geyer A, et al. Identification of viral agents causing diarrhea among children in the Eastern Center of Tunisia. J Med Virol. 2006;78(9):1198-203. • Trabelsi A, Peenze I, Pager C, Jeddi M, Steele D. Distribution of rotavirus VP7 serotypes and VP4 genotypes circulating in Sousse, Tunisia, from 1995 to 1999: emergence of natural human reassortants. J Clin Microbiol. 2000;38(9):3415-9. • Kamel AH, Ali MA, El Nady HG, de Rougemont A, Pothier P, Belliot G. Predominance and circulation of enteric viruses in the region of Greater Cairo, Egypt. J Clin Microbiol. 2009;47(4):1037-45. • Wierzba TF, Abdel-Messih IA, Abu-Elyazeed R, Putnam SD, Kamal KA, Rozmajzl P, et al. Clinic-based surveillance for bacterial- and rotavirus-associated diarrhea in Egyptian children. Am J Trop Med Hyg. 2006;74(1):148-53. • El Mohamady H, Abdel-Messih IA, Youssef FG, Said M, Farag H, Shaheen HI, et al. Enteric pathogens associated with diarrhea in children in Fayoum, Egypt. Diagn Microbiol Infect Dis. 2006;56(1):1-5. • Al Awaidy SA, Bawikar S, Al Busaidy S, Baqiani S, Al Abedani I, Varghesem R. Considerations for introduction of a rotavirus vaccine in Oman: rotavirus disease and economic burden. J Infect Dis. 2009;200(Suppl1):S248-S253. • Al Lawati Z, Al Toubi M. Community health & disease surveillance newsletter Oman. On Ministry of Health Oman website [updated 2008 Oct; cited 2009 Nov 2]. Available from: www.moh.gov.om/reports/publications/Newsletter17-8.pdf. • Marmash RW, Dalwai AK, Szucs G, Molla AM, Pacsa AS, Al Nakib W, et al. Genotypic characterization of rotaviruses and prevalence of serotype-specific serum antibodies in children in Kuwait. Epidemiol Infect. 2007;135(8):1331-7. • Naficy AB, Abu-Elyazeed R, Holmes JL, Rao MR, Savarino SJ, Kim Y, et al. Epidemiology of rotavirus diarrhea in Egyptian children and implications for disease control. Am J Epidemiol. 1999;150(7):770-7. • Eesteghamati A, Gouya M, Keshtkar A, Najafi L, Zali MR, Sanaei M, et al. Sentinel hospital-based surveillance of rotavirus diarrhea in Iran. J Infect Dis. 2009;200 Suppl 1:S244-S247. • Modarres S, Rahbarimanesh AA, Karimi M, Modarres S, Motamedi-Rad M, Sohrabi A, et al. Electrophoretic RNA genomic profiles of rotavirus strains prevailing among hospitalized children with acute gastroenteritis in Tehran, Iran. Arch Iran Med. 2008;11(5):526-31. • Khalili B, Cuevas LE, Reisi N, Dove W, Cunliffe NA, Hart CA. Epidemiology of rotavirus diarrhoea in Iranian children. J Med Virol. 2004;73(2):309-12. • Zarnani AH, Modarres S, Jadali F, Sabahi F, Moazzeni SM, Vazirian F. Role of rotaviruses in children with acute diarrhea in Tehran, Iran. J Clin Virol. 2004;29(3):189-93. • Ali MB, Ghenghesh KS, Aissa RB, Abuhelfaia A, Dufani M. Etiology of childhood diarrhea in Zliten, Libya. Saudi Med J. 2005;26(11):1759-65. • Benhafid M, Youbi M, Klena JD, Gentsch JR, Teleb N, Widdowson M-A, et al. Epidemiology of rotavirus gastroenteritis among children <5 years of age in Morocco during 1 year of sentinel hospital surveillance, June 2006-May 2007. J Infect Dis. 2009;200(Suppl1):S70-S75. • Bozdayi G, Dogan B, Dalgic B, Bostanci I, Sari S, Battaloglu NO, et al. Diversity of human rotavirus G9 among children in Turkey. J Med Virol. 2008;80(4):733-40. • Ceyhan M, Alhan E, Salman N, Kurugol Z, Yildirim I, Celik U, et al. Multicenter prospective study on the burden of rotavirus gastroenteritis in Turkey, 2005-2006: a hospital-based study. J Infect Dis. 2009;200(Suppl1):S234-S238. • Karadag A, Acikgoz ZC, Avci Z, Catal F, Gocer S, Gamberzade S, et al. Childhood diarrhoea in Ankara, Turkey: epidemiological and clinical features of rotavirus-positive versus rotavirus-negative cases. Scand J Infect Dis. 2005;37(4):269-75. • Kurugol Z, Geylani S, Karaca Y, Umay F, Erensoy S, Vardar F, et al. Rotavirus gastroenteritis among children under five years of age in Izmir, Turkey. Turk J Pediatr. 2003;45(4):290-4. • Muhsen K, Shulman L, Rubinstein U, Kasem E, Kremer A, Goren S, et al. Incidence, characteristics, and economic burden of rotavirus gastroenteritis associated with hospitalization of Israeli children <5 years of age, 2007-2008. J Infect Dis. 2009;200(Suppl1):S254-S263. • Ahmed HM, Coulter JB, Nakagomi O, Hart CA, Zaki JM, Al Rabaty AA, et al. Molecular characterization of rotavirus gastroenteritis strains, Iraqi Kurdistan. Emerg Infect Dis. 2006;12(5):824-6. • Cunliffe NA, Dove W, Bunn JE, Ben Ramadam M, Nyangao JW, Riveron RL, et al. Expanding global distribution of rotavirus serotype G9: detection in Libya, Kenya, and Cuba. Emerg Infect Dis. 2001;7(5):890-2. • Villena C, El Senousy WM, Abad FX, Pinto RM, Bosch A. Group A rotavirus in sewage samples from Barcelona and Cairo: emergence of unusual genotypes. Appl Environ Microbiol. 2003;69(7):3919-23. • Cataloluk O, Iturriza M, Gray J. Molecular characterization of rotaviruses circulating in the population in Turkey. Epidemiol Infect. 2005;133(4):673-8. • Ciftci E, Tapisiz A, Ozdemir H, Guriz H, Kendirli T, Ince E, et al. Bacteraemia and candidaemia: A considerable and underestimated complication of severe rotavirus gastroenteritis. Scand J Infect Dis. 2009;1-5. • World Health Organization. Child rotavirus deaths . On World Health Organization website [updated 2004; cited 2009 Nov 2]. Available from: http://www.who.int/immunization_monitoring/burden/rotavirus_estimates/en/index.html. • UNICEF. Information by country and programme - Demographic indicators. On UNICEF website [updated 2004 Feb 26; cited 2009 Dec 11]. Available from: http://www.unicef.org/infobycountry/index.html. • Samarbafzadeh A, Tehrani EM, Makvandi M, Taremi M. Epidemiological aspects of rotavirus infection in Ahwaz, Iran. J Health Popul Nutr. 2005;23(3):245-9. • Williams CJ, Lobanov A, Pebody RG. Estimated mortality and hospital admission due to rotavirus infection in the WHO European region. Epidemiol Infect. 2009;137(5):607-16. • Waisbourd-Zinman O, Ben Ziony S, Solter E, Scherf E, Samra Z, Ashkenazi S. Hospitalizations for nosocomial rotavirus gastroenteritis in a tertiary pediatric center: a 4-year prospective study. Am J Infect Control. 2009;37(6):465-9. • Youssef M, Shurman A, Bougnoux M, Rawashdeh M, Bretagne S, Strockbine N. Bacterial, viral and parasitic enteric pathogens associated with acute diarrhea in hospitalized children from North Jordan. FEMS Immunol Med Microbiol. 2000;28(3):257-63. • Conclusions • RVGE is a common disease resulting in significant morbidity, mortality, and costs in the Middle East and North Africa. • Study limitations that restricted comparability of data across countries are: limited availability of recent serotype information in some countries and wide variation in time frames; variations in study setting and design. In addition, limited data availability on RVGE mortality, morbidity, and economic burden restricted the evaluation of RVGE global burden for the region. • A vaccine with broad and consistent serotype coverage would be important to help decrease the burden of RVGE in the region.






