Download
1 / 19
210 likes | 544 Views
Pharmacokinetics of Paromomycin (Aminosidine) in Healthy Volunteers and Kala-azar Patients M.M.E. Mudawi 1, 2 , E.A.G. Khalil 2 , I.B. Eltayeb 3 , A.M. Musa 2 , S.A.I. Shaddad 3 , Isaiah M.Githiga 4 , G.O. Kokwaro 4, 5 1- Faculty of Pharmacy, Omdurman Islamic University, Sudan.

E N D
Pharmacokinetics of Paromomycin (Aminosidine) in Healthy Volunteers and Kala-azar Patients M.M.E. Mudawi1, 2, E.A.G. Khalil2, I.B. Eltayeb3, A.M. Musa2, S.A.I. Shaddad3, Isaiah M.Githiga4, G.O. Kokwaro4, 5 1- Faculty of Pharmacy, Omdurman Islamic University, Sudan. 2- Leishmaniasis Research Group, Institute of Endemic Diseases, University of Khartoum, Sudan. 3- Faculty of Pharmacy, University of Khartoum, Sudan. 4- Department of Pharmaceutics and Pharmacy Practice, School of Pharmacy, University of Nairobi, Nairobi, Kenya. 5- Kenya Medical Research Institute (KEMRI)/Wellcome Trust Research Programme, Centre for Geographic Medicine Research (Coast), Kenya. Presenter: Mahmoud Mudawi El tahir
Introduction: • Currently the main foci of visceral leishmaniasis are in Sudan and India and those of cutaneous leishmaniasis are in Afghanistan, Syria, and Brazil (Simon; et al., 2006). • Current treatments of visceral leishmaniasis are far from satisfactory; they are either toxic or expensive. Moreover, some may require long courses and parenteral administration. (Karin and Simon; 2006). • There is an urgent need for development of combination therapies to prevent drug resistance, reduce cost and toxicity of longer courses of monotherapy. However, research and development in leishmania has been neglected, because the disease mainly affects the poor sector. (Philippe; et al., 2002).
Introduction… • Paromomycin is an aminoglycoside antibiotic identical to aminosidine. • An injectable formulation of 500 mg of paromomycin sulphate had until recently been on the market in several countries for over 35 years for the treatment of bacterial and parasitic infections (Thakur and co-workers, 2000). • Aminosidine was first shown to have antileishmanial activity in the 1960s, and it has been shown to act synergistically with antimony drugs (Jha; et al., 1998).
Introduction… • Like other aminoglycoside antibiotics aminosidine is poorly absorbed from the gastro-intestinal tract. Aminosidine binds to serum proteins to a limited extent and is eliminated unchanged through the kidneys (Scott; et al., 1992). • As part of a multicentre trial of the efficacy and safety of paromomycin sulfate (PM) and sodium stibogluconate (SSG) in the treatment of visceral leishmaniasis, the pharmacokinetics of the paromomycin was studied in healthy volunteers and kalazar patients in order to relate drug disposition profile to safety.
Objectives: • 1- To study the pharmacokinetics of Paromomycin (PM) in patients suffering from visceral leishmaniasis and in healthy volunteers in Sudan. • 2- To study the effects of visceral leishmaniasis (VL) on Paromomycin pharmacokinetics. • The pharmacokinetic study was performed as follows: • 1- An initial assay development and validation phase. • 2- Assay of paromomycin in urine and plasma, followed by pharmacokinetic analysis.
Study design: • A cross sectional study was conducted as part of the dose finding study of paromomycin that was conducted in Kassab hospital (15 mg/kg i.m for 28 days Vs 20 mg/kg i.m for 21 days)(Musa et al., 2010). • The study received an ethical clearance from the ministry of health,(Sudan).
Methods: • Patients and healthy volunteers were enrolled after they have agreed to participate in the study and signed a written informed consent form. • Blood and urine samples collection: • A- Patients: • Venous blood samples were collected in heparinized tubes at 15, 30 minutes and 1, 2, 4, 6, 8, 12 and 24 hours after administration of paromomycin (PM). Blood samples were collected at the same intervals at day 14 of treatment for the group given Paromomycin 20 mg/kg and at day 28 of treatment for the group given Paromomycin 15 mg/kg. • Urine samples were collected during 0 to 2, 2 to 4, 4 to 6, 6 to 8, 8 to 12, and 12 to 24 hours. The total urine volume for each interval was recorded and aliquot was stored until assay. Urine samples were also collected at the same intervals at day 14 and the last day of treatment.
Methods… • B- Healthy volunteers: • Venous blood samples were collected in heparinized tubes at 15, 30 minutes and 1, 2, 4, 6, 8, 12 and 24 hours after administration of Paromomycin (PM). • Urine samples were collected during 0 to 2, 2 to 4, 4 to 6, 6 to 8, 8 to 12, and 12 to 24 hours. The total urine volume for each interval was recorded and aliquot was stored until assay.
Methods… • Assay and Pharmacokinetic analysis: • The analysis of plasma and urine sample was performed with a high-performance liquid chromatographic (HPLC). • Mean concentrations at each sampling point were determined for both patients and volunteers. In addition, for volunteers, plasma drug concentration-time profiles were fit into a non compartmental pharmacokinetics model for drug disposition following IM administration, using the pharmacokinetic programmeKinetica 4.4. • The cumulative amounts excreted in urine were expressed as percentage of the dose administered.
Results: • Table (1): Comparison of the mean ± (SD) plasma conc. (µg/ml) for patients receiving Paromomycin 15 mg/kg i.m on Day 1 and Day 26: ( P < 0.05 * significant difference)
Results… • Table (2): Comparison of the mean ± (SD) plasma conc. (µg/ml) for patients receiving Paromomycin 20 mg/kg i.m on Day 1 and Day 14: ( P < 0.05 * significant difference)
Results… • Table (3): Comparison of the mean ± (SD) plasma conc. (µg/ml) for patients receiving Paromomycin 15 mg/kg i.m and 20 mg/kg i.m: ( P < 0.05 * significant difference)
Results… • Table (4): Comparison of the mean ± (SD) plasma conc. (µg/ml) for patients receiving Paromomycin 15 mg/kg i.m on day 1 and volunteers (15 mg/kg single dose): ( P < 0.05 * significant difference)
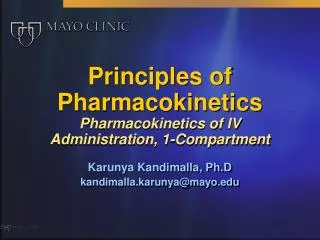
25 20 volunteers single 15 patients 15(D1) Aminosidine concentration (ug/ml) patients 15(D26) patients 20(D1) 10 patients 20(D14) 5 0 0.25 0.5 1 2 4 6 8 Time(hours) • Results… • Figure 1: Curves of mean Paromomycin concentration in plasma form volunteers receiving Paromomycin 15 mg/kg (single dose) and patients receiving Paromomycin (15 mg/kg (D1, D26) and 20 mg/kg (D1, D26)):
Results… • In general, peak Paromomycin concentrations were achieved within 2 hours both in patients and volunteers. • Mean Paromomycin concentrations on day1 were not significantly different from those on day 26, and on day1 and day14 following administration of 15 mg/kg and 20 mg/kg dose, respectively, to patients. • Similarly, there were no significant differences between mean Paromomycin plasma concentrations in patients administered the 15 mg/kg dose and those administered the 20 mg/kg dose (day1 versus day1). However, mean Paromomycin concentrations in volunteers who received the single 15 mg/kg dose were, in general, significantly higher than day1 and day 26 mean concentrations in patients who received the 15 mg/kg multiple doses. • Most of the administered dose was excreted in the urine of patients and volunteers within 24 hours.
Discussion: • In this study there were no significant differences between the serum level of Paromomycin (PM) 15 mg (day 1 & day 26) and 20 mg (day 1 & day 14) but the level of PM 20 mg appeared to be higher that means there is no accumulation ( no trough) so there is a possibility that PM can be given more than once. • The percentage of the dose was recovered completely in urine within 24 hours, suggested that absorption was complete in these patients and volunteers.
Discussion… • In line with the study conducted by Kanyok (Kanyok; et al., 1997) in America on healthy volunteers our healthy volunteers showed the same pharmacokinetic pattern as those in America, this indicate that there is no genetic effect on the pharmacokinetic profile of PM. • On the other hand our VL patients showed lower concentrations of PM probably because of the hyperdynamics circulation (because VL patients are anemic, febrile and with oragnomegally).
Conclusion: • The injected concentration determines the plasma level of PM. • The hyperdynamics circulation observed in VL patients resulted in lower plasma concentration of PM compared with healthy volunteers. • The peak level concentration of PM was attained 2 hours following i.m administration. • The percentage of the dose that was recovered completely in urine within 24 hours, suggested that absorption was complete in these patients and volunteers.
ACKNOWLEDGEMENT: • This work was supported by: Drugs for Neglected Diseases initiative (DNDi).