Download
1 / 1
10 likes | 272 Views
No. 049. Necrotizing fasciitis of anterior abdominal wall from a prostatic abscess: A previously unreported complication. David Low, Richard McMullin , Tom Fisher, Cherng Huei Kong, Emma Tully, Brionny Norriss Ballarat Base Hospital Victoria 2012. Posters Proudly Supported by: .

E N D
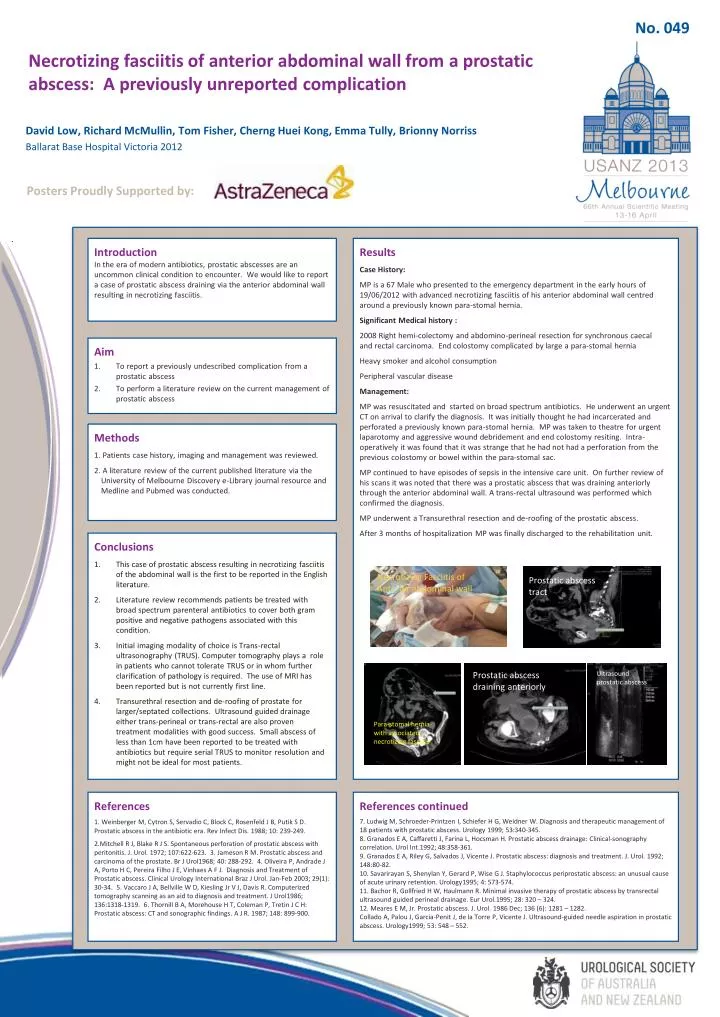
No. 049 Necrotizing fasciitis of anterior abdominal wall from a prostatic abscess: A previously unreported complication David Low, Richard McMullin, Tom Fisher, CherngHuei Kong, Emma Tully, BrionnyNorriss Ballarat Base Hospital Victoria 2012 Posters Proudly Supported by: Introduction In the era of modern antibiotics, prostatic abscesses are an uncommon clinical condition to encounter. We would like to report a case of prostatic abscess draining via the anterior abdominal wall resulting in necrotizing fasciitis. Results Case History: MP is a 67 Male who presented to the emergency department in the early hours of 19/06/2012 with advanced necrotizing fasciitis of his anterior abdominal wall centred around a previously known para-stomal hernia. Significant Medical history: 2008 Right hemi-colectomy and abdomino-perineal resection for synchronous caecal and rectal carcinoma. End colostomy complicated by large a para-stomal hernia Heavy smoker and alcohol consumption Peripheral vascular disease Management: MP was resuscitated and started on broad spectrum antibiotics. He underwent an urgent CT on arrival to clarify the diagnosis. It was initially thought he had incarcerated and perforated a previously known para-stomal hernia. MP was taken to theatre for urgent laparotomy and aggressive wound debridement and end colostomy resiting. Intra-operatively it was found that it was strange that he had not had a perforation from the previous colostomy or bowel within the para-stomal sac. MP continued to have episodes of sepsis in the intensive care unit. On further review of his scans it was noted that there was a prostatic abscess that was draining anteriorly through the anterior abdominal wall. A trans-rectal ultrasound was performed which confirmed the diagnosis. MP underwent a Transurethral resection and de-roofing of the prostatic abscess. After 3 months of hospitalization MP was finally discharged to the rehabilitation unit. Aim To report a previously undescribed complication from a prostatic abscess To perform a literature review on the current management of prostatic abscess Methods 1. Patients case history, imaging and management was reviewed. 2. A literature review of the current published literature via the University of Melbourne Discovery e-Library journal resource and Medline and Pubmed was conducted. Conclusions This case of prostatic abscess resulting in necrotizing fasciitis of the abdominal wall is the first to be reported in the English literature. Literature review recommends patients be treated with broad spectrum parenteral antibiotics to cover both gram positive and negative pathogens associated with this condition. Initial imaging modality of choice is Trans-rectal ultrasonography (TRUS). Computer tomography plays a role in patients who cannot tolerate TRUS or in whom further clarification of pathology is required. The use of MRI has been reported but is not currently first line. Transurethral resection and de-roofing of prostate for larger/septated collections. Ultrasound guided drainage either trans-perineal or trans-rectal are also proven treatment modalities with good success. Small abscess of less than 1cm have been reported to be treated with antibiotics but require serial TRUS to monitor resolution and might not be ideal for most patients. Necrotizing Fasciitis of Anterior abdominal wall Prostatic abscess tract Ultrasound prostatic abscess Prostatic abscess draining anteriorly Para-stomal hernia with associated necrotizing fasciitis References 1. Weinberger M, Cytron S, Servadio C, Block C, Rosenfeld J B, Putik S D. Prostatic abscess in the antibiotic era. Rev Infect Dis. 1988; 10: 239-249. 2.Mitchell R J, Blake R J S. Spontaneous perforation of prostatic abscess with peritonitis. J. Urol. 1972; 107:622-623. 3. Jameson R M. Prostatic abscess and carcinoma of the prostate. Br J Urol1968; 40: 288-292.4. Oliveira P, Andrade J A, Porto H C, Pereira Filho J E, Vinhaes A F J. Diagnosis and Treatment of Prostatic abscess. Clinical Urology International Braz J Urol. Jan-Feb 2003; 29(1): 30-34.5. Vaccaro J A, Bellville W D, KieslingJr V J, Davis R. Computerized tomography scanning as an aid to diagnosis and treatment. J Urol1986; 136:1318-1319.6. Thornill B A, Morehouse H T, Coleman P, Tretin J C H: Prostatic abscess: CT and sonographic findings. A J R. 1987; 148: 899-900. References continued 7. Ludwig M, Schroeder-Printzen I, Schiefer H G, Weidner W. Diagnosis and therapeutic management of 18 patients with prostatic abscess. Urology 1999; 53:340-345. 8. Granados E A, Caffaretti J, Farina L, Hocsman H. Prostatic abscess drainage: Clinical-sonography correlation. Urol Int.1992; 48:358-361. 9. Granados E A, Riley G, Salvados J, Vicente J. Prostatic abscess: diagnosis and treatment. J. Urol. 1992; 148:80-82. 10. Savarirayan S, Shenylan Y, Gerard P, Wise G J. Staphylococcus periprostatic abscess: an unusual cause of acute urinary retention. Urology1995; 4: 573-574. 11. Bachor R, Gollfried H W, Haulmann R. Minimal invasive therapy of prostatic abscess by transrectal ultrasound guided perineal drainage. Eur Urol.1995; 28: 320 – 324. 12. Meares E M, Jr. Prostatic abscess. J. Urol. 1986 Dec; 136 (6): 1281 – 1282. Collado A, Palou J, Garcia-Penit J, de la Torre P, Vicente J. Ultrasound-guided needle aspiration in prostatic abscess. Urology1999; 53: 548 – 552.






