Download
1 / 12
130 likes | 735 Views
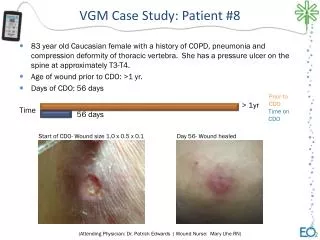
Homerton Hospital Case Study of a stroke patient. By Sarah Hart Student no’s 0604985. Introduction. 80yr old gentlemen BIBA (brought in by ambulance) to Royal London Hospital (RLH) after a fall on the 12/12/07. No loss of consciousness

E N D
Homerton HospitalCase Study of a stroke patient. By Sarah Hart Student no’s 0604985
Introduction • 80yr old gentlemen BIBA (brought in by ambulance) to Royal London Hospital (RLH) after a fall on the 12/12/07. • No loss of consciousness • Diagnosis- Right CVA (cerebral vascular accident), mild lacunar infarct of the basal ganglia bilaterally.
Cerebral vascular accident (CVA) • Definition- By the WHO as ‘rapidly developing clinical signs of focal cerebral function with symptoms lasting no more than 24hrs or leading to death, with no apparent cause other than the vascular origin’ (Smith 1997) • Lacunar infarct- Lacunar stroke occurs when one of the small arteries that provide blood to the brain's deep structures is blocked and injure deeper structures underneath the cortex.
Previous Medical History (PMH) • Diabetic type II • Hypertension • Bilateral renal cyst • LVF (EF 28%) • Hyperlipidaemia • TURP (transurethral resection of the prostate)
Social History (SH) • Lives in a maisonette with his wife. • Stairs indoors and out. Bathroom and bedroom upstairs. • Council rented • Ex-smoker. • Prior to admission, independently mobilising, no problems with ADL’s and communication.
Report from RLH • 8x12m mobilising with a quad stick. • Sit-stand with supervision • AO1 to get from laying-SOEOB • Requires prompt to pick up (L) leg during gait.
Right UL -NAD Left UL- AROM- some selective activity PROM- decreased at GHJ, wrist and elbow. Tone- Distally low tone Proprioception- Normal Co-ordination- unable to assess Right LL- NAD Left LL- Hip and Knee flexion present grade 3 Co-ordination impaired (muscle weakness) OA Homerton Hospital
Functional tasks • Bed mobility- AO2. • Transfer- AO2. • Sit-Stand Independent. • Gait is unsteady. • Balance is reduced. • Unsafe during turning around when mobilising. • Rivermead score 17
Initial Goal • Using the GAS (Goal Attainment Scale) • His transfer goals were to progress to transferring from laying in bed to sitting on the edge of the bed by himself • His mobility goals were to mobilise with a stick independently. Both goals were discussed with the patient.
Therapy sessions • Practising transfers. • Practising mobilising with quadstick and walking stick. • Increasing exercise tolerance.
Long term Goals • Mobilising independently with a stick. • Be able to walk up and down the stairs safely.
References • http://www.stroke.org.nz/assets/ischaemic_stroke_sml.gifwww.stroke.org.nz • Smith, M.T., Baer, G.D., (1997). Measuring the outcomes for specific stroke sub-types using simple mobility milestones, Physiotherapy, 83, 254