Download
1 / 26
260 likes | 331 Views
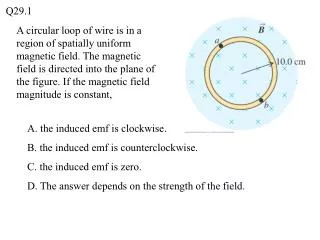
Does Transdermal Nicotine-Induced Withdrawal Suppression Depend on Smokers’ Gender?. Sarah E. Evans, Ph.D. Seminars in Addiction Psychiatry October 6, 2005. Acknowledgments. NIH: R01 DA11082 T32 DA 07027 Research staff: Cynthia Sams, R.N., Melodie Anderson, R.N.

E N D
Does Transdermal Nicotine-Induced Withdrawal Suppression Depend on Smokers’ Gender? Sarah E. Evans, Ph.D. Seminars in Addiction Psychiatry October 6, 2005
Acknowledgments. • NIH: • R01 DA11082 • T32 DA 07027 • Research staff: • Cynthia Sams, R.N., Melodie Anderson, R.N. • Robert James Collins, Kasha White, Jenny Gray, Tom Campbell, Amy Opilla and Tamika Gilreath • Lynn Anderson, Melissa Blank, Alison Breland and Annie Kleykamp • Michael Weaver, M.D. • Randy James, Ph.D. • Thomas Eissenberg, Ph.D.
Overview. • Smoking kills >400,000 Americans/year. • Quitting smoking reduces risk of tobacco-related death and disease. • Several medications, including nicotine replacement (e.g., transdermal nicotine or TN) help smokers quit. • Medication (including TN) efficacy thought to be based on suppression of nicotine/tobacco withdrawal during abstinence. • Even with medication, lower quit rates for women are observed. • Lower quit rates for women may reflect less medication-induced withdrawal suppression. • Introductory topics include: Clinical evidence for nicotine reinforcement and withdrawal, NRT’s efficacy and withdrawal suppression, gender differences in response to NRT.
Clinical evidence for reinforcement and withdrawal. • Nicotine is a reinforcer in humans • Robust self-administration of pure nicotine and tobacco-delivered nicotine. • After discontinuation of chronic tobacco-delivered nicotine: • Signs such as reduced heart rate, increased caloric intake and weight, change in EEG frequency • Behavioral performance decrements such as decreased concentration, impaired attention • Symptoms such as urge to smoke, impatient, irritability, difficulty concentrating • Withdrawal syndrome can reduce the likelihood of a quit attempt and decrease chances of long-term cessation.
Pharmacologically Pure Nicotine is Efficacious. • Nicotine replacement therapy (NRT): Gum, transdermal, lozenge, inhaler, and nasal spray • Approximately doubles long-term cessation rates • Thought to work, at least in part, via withdrawal suppression (i.e., reduced urge to smoke, impatient, irritability, difficulty concentrating). • NRT-induced withdrawal suppression has been demonstrated with every formulation.
Transdermal nicotine suppresses withdrawal effects: • Decreased heart rate • Changes in brain activity • Weight gain • Decreased performance • Urge to smoke, impatient, irritability, difficulty concentrating
Gender differences in response to nicotine & NRT. • Gender differences in response to NRT: laboratory evaluations • pain sensitivity • self-administration • Gender differences in response to NRT: clinical trials • Many trials report lower cessation rates for women (Bjornson et al., 1995; Wetter et al., 1995;TNSG, 1991) • No trials have shown lower cessation rates for men. • Gender differences NRT-induced withdrawal suppression? • Greater impatience, hunger for women (Hatsukami et al., 1995). • Craving suppressed for men only (Killen et al., 1990). • Better sleep efficiency for men (Wetter et al., 1999).
Detecting gender differences: design issues. • Power (N = 34, Wetter et al., 1999). • Dose (no placebo dose, Hatsukami et al., 1995; single dose, Wetter et al., 1999; Killen et al., 1990). • Outcome measures (symptom checklists instead of standardized measures, Hatsukami et al., 1995).
Purpose. To determine if TN-induced withdrawal suppression is influenced by smokers’ gender in a large sample of men and women, across a variety of TN doses, and using standardized measures of tobacco/nicotine withdrawal.
Method. • Within subject (crossover) design; N = 128. • Four, double-blind, Latin square-ordered, 6.5-hour sessions. • The sessions corresponded to four TN doses (0, 7, 21, 42 mg). • 8+ hours pre-session abstinence, verified by CO < 10ppm. • Plasma nicotine, heart rate, and subjective withdrawal assessed regularly in each session. • Women participants scheduled only during days 2 – 16 of their menstrual cycle.
Inclusion/exclusion criteria. • Inclusion: • Smokers of any “king size” or “100s” cigarettes. • Between 18-55 years of age. • Afternoon expired air carbon monoxide (CO) >15 ppm. • Reported smoking > 15 cigs/day for past 2 years. • Exclusion: • Pregnant or breast feeding. • History of chronic psychiatric or health problems. • Score > 17 on BDI (abstinence exacerbates depression)
Outcome measures. • Physiological effects • Plasma nicotine level assessed each hour. • Heart rate recorded continuously (30 minute bins). • Subjective effects assessed each hour: • Hughes-Hatsukami (1986) withdrawal symptom VAS. • Tiffany-Drobes (1991) Questionnaire of Smoking Urges (QSU). • Direct effects visual analog scale (VAS).
Subjective measure: Hughes-Hatsukami VAS. URGES to smoke Extremely Not at all Anxious Extremely Not at all CRAVING a cigarette/nicotine Extremely Not at all
Subjective measure: QSU. I need a cigarette now Strongly disagree Strongly agree Smoking a cigarette would not be pleasant Strongly disagree Strongly agree My desire to smoke seems overwhelming Strongly disagree Strongly agree
Subjective measure: Direct Effects VAS. Nauseous Extremely Not at all Dizzy Extremely Not at all Lightheaded Extremely Not at all
Session procedure. Plasma Nicotine B B B B B B B Subjective S S S S S S S 1 0 2 4 5 6 3 Time in hours Patch Administration (0, 7, 21 or 42 mg)
Participant characteristics. CharacteristicMen (N= 75)Women (N= 53) Non-white (%) 49 51 Mean age [SD] 35.4 [10.2] 32.3 [10.4] Mean cigarettes per/day 24.1 [10.0]21.3 [5.8] Duration cigarette use 13.0 [9.3]9.1 [7.4]* Mean Fagerström NTQ [SD]1 5.8 [2.2] 5.1 [2.0] Mean quit attempts [SD] 4.0 [7.4] 2.6 [2.5] Previous patch use (%) 25 25 1Max score = 11
Active patch suppressed Craving and Urges. 42 42 21 21 Craving VAS Craving VAS Urges to Smoke VAS Urges to Smoke VAS 7 7 0 0 100 100 60 60 40 40 Score Score * * * * 20 20 0 0 0 0 60 60 120 120 180 180 240 240 300 300 360 360 0 0 60 60 120 120 180 180 240 240 300 300 360 360 Time in minutes, relative to patch administration Time in minutes, relative to patch administration Time in minutes, relative to patch administration Time in minutes, relative to patch administration
Active patch suppressed Craving and Urges. Men Women Craving VAS Urges to Smoke VAS 100 60 40 * Score * 20 0 0 7 21 42 0 7 21 42 Transdermal nicotine dose (mg) Transdermal nicotine dose (mg)
Men Women DSM-IV items suppressed, not dose-related. Irritability/Frustration/Anger VAS 100 40 30 20 10 0 0 7 21 42 Transdermal nicotine dose (mg)
Men Women Some patch doses produced aversive effects. Dizzy VAS Nauseous VAS 100 25 + * + * 20 15 * Score * 10 5 0 0 7 21 42 0 7 21 42 Transdermal nicotine dose (mg) Transdermal nicotine dose (mg)
Men Women Few gender effects. Men Men Women Women Lightheaded VAS Lightheaded VAS QSU Factor 1 QSU Factor 1 100 90 ‡ ‡ 80 + + 25 25 * * 70 70 ‡ ‡ * * 20 20 60 60 + + * * 50 50 Score Score 15 15 Score Score 40 40 30 30 10 10 20 20 5 5 10 10 0 0 0 0 7 21 0 42 0 0 21 21 42 42 7 7 Transdermal nicotine dose (mg) Transdermal nicotine dose (mg) Transdermal nicotine dose (mg)
Summary • Clear dose-related effects for plasma nicotine and heart rate. • Clear dose-related suppression for Craving and Urges to Smoke. • Many DSM-IV nicotine/tobacco withdrawal symptoms were suppressed by active TN, but this suppression was not dose-related (e.g. Irritability/Frustration/Anger, Anxious, Difficulty Concentrating). • Highest TN dose (42 mg) produced reliable, aversive effects such as nausea, lightheadedness and dizziness. • Very few outcome measures were influenced by smokers’ gender. • Limitations include non-treatment seeking sample and acute, laboratory-based design.
Future research interests. • Clear dose-related effects for plasma nicotine and heart rate. • Assessing smoking characteristics of MA users • CReSSMicro