Download
1 / 30
350 likes | 776 Views
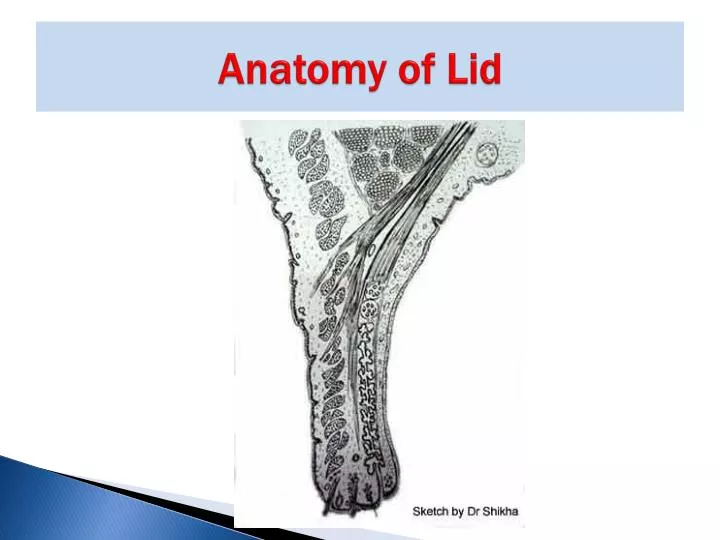
Anatomy of Lid. Blepharitis. Blepharitis. Blepharitis is chronic inflammation of lid margin occurring as true inflammation or as simple hyperaemia. (Very common cause of ocular discomfort and irritation). Types. 1. Anterior a. Squamous b. Ulcerative 2. Posterior

E N D
Blepharitis Blepharitis is chronic inflammation of lid margin occurring as true inflammation or as simple hyperaemia. (Very common cause of ocular discomfort and irritation)
Types 1. Anterior a. Squamous b. Ulcerative 2. Posterior a. Meibomian seborrhoea b. Meibomianitis (Conditions overlap with each other)
Causes • Following chronic Conjunctivitis especially due to staphylococci • Phthiriasis Palpabrarum due to crab louse (Poor correlation between signs and symptoms, uncertain etiology and mechanism)
Seborrhoeic or SquamousBlepharitis • Is a form of anterior blebharitis characterized by deposition of white scales among the eye lashes. Eye lashes fall and replaced by distorted eyelashes. • On removal of scales, lid margins appear hyperaemic. Ulcers are absent.
Seborrhoeic or SquamousBlepharitis • Condition is metabolic associated with dandruff of the scalp • Usually associated with seborrhoeic dermatitis involving scalp, nasolabial folds and retroauricular areas
Symptoms • Burning, grittiness , redness of lid margins, mild photophobia • Symptoms are worse in the morning (Remissions and exacerbations)
Seborrhoeic or SquamousBlepharitisTreatment • Skin and Scalp condition also requires treatment. • Lid Hygiene • Hot compresses • Topical Antibiotics • Oral Azithromycin 500 mg daily for 3 days • Weak topical steroids (Flourometholone) • Tear Substitutes
Staphylococcal or Ulcerative Blepharitis • Ulcerative blepharitis is infective condition commonly due to staphylococcal infection (Cell mediated response) • Lid margins are covered with infective material (yellow crusts or dry brittle scales-Collarettes) matting eyelashes. • On removal of discharge small ulcers which bleed are found along lid margins around bases of the eyelashes
Symptoms • Redness of lid margins, burning, itching, watering and photophobia • Signs: • Small ulcers at lid margins on removal of discharge, this feature differentiate it from conjunctivitis
Treatment • Discharge/ crust is removed from lid margins with 1:4 dilution baby shampoo or luke warm 3% soda bicarbonate lotion. The loose discharge is then cleaned cotton • Diseased eyelashes are epilated
Treatment • Appropriate antibiotic drops are used • After control of infection, daily cleaning of lid margins with blend lotion
Treatment • Improvement of local hygiene (rubbing of eyes and touching of eyes with dirty hand should be discouraged)
Sequelae of Ulcerative Blepharitis • Chronic course and associated chronic conjunctivitis & Marginal Keratitis • Madarosis (Scanty eyelashes) due to falling of eyelashes • Poliosis (Whitening)
Sequelae of Ulcerative Blepharitis • Trichiasis (misdirected eyelashes) due to contraction of scar tissue • Cicatrization of lid margins causing thickening and hypertrophy of tissue and drooping of lids (Tylosis)
Sequelae of Ulcerative Blepharitis • Cicatrization of lid margin may drag conjunctiva on posterior border of intermarginal strip disturbing angle of posterior edge leading to epiphora , eversion of puncta • Epiphora leads to eczematous condition of skin, scarring of skin leads to ectropion . This further aggravate epiphora • Tear film instability
Posterior Blepharitis • Posterior blepharitis i.e. inflammation of meibomian duct opening at intermarginal strip and posterior border may cause tear film instability and inferior punctate keratitis
Posterior Blepharitis • Meibomian gland dysfunction and alterations in meibomian gland secretion • Bacterial lipases may result in the formation of fatty acids which may lead to increase in melting point of meibum
Posterior Blepharitis • Caping with Oil globules • Plugging • Hyperemia • Teengiectasis
Posterior Blepharitis It occurs in two clinical forms • Meibomianseborrhoea • Meibomianitis
Meibomianseborrhoea 1. Meibomian seborrhoea – characteristic appearance of oil droplet at the opening of meibomian duct opening at intermarginal strip. Tear film is oily and foamy. Frothy discharge accumulate on the lid margin. Foam like discharge can be expressed from these lesions
Meibomianitis 2. Meibomianitis – There is inflammation and obstruction of meibomian glands. Characterized by diffuse thickening of posterior border of lid margin which becomes rounded. On lid massage toothpaste like thick material can be expressed out. Due to duct blockade cyst formation may be present
Complications • Chalazion • Tear film instability • Papillary conjunctivitis and inferior corneal erosions
Treatment • Warm compresses • Systemic - Doxycycline 100 mgm twice x 1 week then once daily for 6 -12 weeks or Tetracycline 250 mgm 4 times x 1 week then twice for 6 -12 weeks • Associated tear film abnormality is treated with artificial tear drops








![Download [PDF] Encyclopedia of Exercise Anatomy (Anatomy of)](https://cdn7.slideserve.com/12559512/slide1-dt.jpg)