Download

1 / 40
400 likes | 451 Views
FOLIC ACID. FOLIC ACID FOLACIN VIT.M VIT .B -9 PTERYLGLUTAMIC ACID. Introduction. Folic acid belongs to water soluble B vitamins. All B vitamins help the body convert food (carbohydrates) into fuel (glucose), which is used to produce energy.

E N D
FOLIC ACID FOLIC ACID FOLACIN VIT.M VIT .B -9 PTERYLGLUTAMIC ACID
Introduction • Folic acid belongs to water soluble B vitamins. • All B vitamins help the body convert food (carbohydrates) into fuel (glucose), which is used to produce energy. • These B vitamins, often referred to as B-complex vitamins, also help the body use fats and protein.
B-complex vitamins are needed for a healthy liver, and healthy Skin, Hair, Nails and Vision. • They also help the nervous system function properly. • Folic acid is the synthetic form of B9, • Found in supplements and fortified foods, • While folate occurs naturally in foods.
Important Role • It aids in the production of DNA and RNA, the body's genetic material, and is especially important when cells and tissues are growing rapidly, such as in infancy, adolescence, and pregnancy. • Folic acid also works closely with vitamin B12 to help make red blood cells and help iron work properly in the body. • Folic acid is crucial for proper brain function and plays an important role in mental and emotional health.
Important Role • Vitamin B9 works with vitamins B6 and B12 and other nutrients to control blood levels of the amino acid homocysteine. • High levels of homocysteine is considered to be closely associated with heart disease. • Whether homocysteine is a cause of heart disease or just a marker that indicates someone may have heart disease, we are not yet quite sure.
HISTORY • In the 1920s, scientists believed folate deficiency and anemia were the same condition. • In 1931, researcher LUCY WILLS made a key observation that led to the identification of folate as the nutrient required to prevent anemia during pregnancy. • Dr. Wills demonstrated that anemia could be reversed with yeast. • In the late 1930s, folate was identified as the corrective substance in yeast.
HISTORY • It was first isolated and extracted from SPINACH leaves by Mitchell and others in 1941. • Bob Stokstad isolated the pure crystalline form in 1943, and was able to determine its chemical structure while working at the Lederle Laboratories of the American Cyanamid Company. • This historical research project, of obtaining folic acid in a pure crystalline form in 1945, was done by the team called the "folic acid boys,”, at the Lederle Lab, Pearl River, NY.
Later on • This research led to the synthesis of the antifolate aminopeptin, the first-ever anticancer drug, the clinical efficacy was proven by Sidney Farber in 1948. • In the 1950s and 1960s, scientists began to discover the biochemical mechanisms of action for folate.
In 1960, experts first linked folate deficiency to neural tube defects(NTD). • In the late 1990s, US scientists realized, despite the availability of folate in foods and in supplements, there was still a challenge for people to meet their daily folate requirements, which is when the US implemented the folate fortification program.
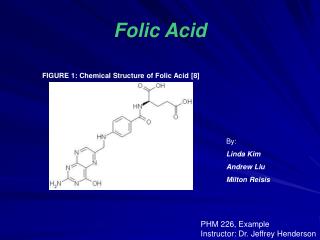
Folacin is generic name for folic acid and related compounds. The chemical term for folacin or folic acid is pteroylglutamic acid.
STRUTURE Folic acid is a conjugated molecule consisting of a pteridine ring structure linked to para-aminobenzoic acid (PABA) that forms pteroic acid. Folic acid is then generated through the conjugation of glutamic acid residues to pteroic acid
COENZYME FORMS OF FOLIC ACID • Positions 7 & 8 carry hydrogen , in Dihydrofolate (DHF) • Positions 5,6,7 and 8 carry hydrogen, in Tetrahydrofolate (THF)
Food Sources • The richest sources of folacin include • Liver • Spinach • Wheat • Yeast and • Dry beans • Almost all deep green leafy vegetables are good sources of this vitamin
Distribution in Body • Total body contents • 6-10 mg • 60% present in Liver. • In plasma up to 20 ng/ml bound to protein • Whole blood level is upto 300 ng/ml Excretion is through urine, feces and bile.
Absorption and Metabolism • Plants Folic Acid contains 7 or 5 Glutamyl Residues linked together by a peptide bond. • The peptide bond is hydrolyzed by intestinal enzymes and the compound with one glutamyl residues is formed • Folic acid in this monoglutamyl form is absorbed only. • It is then reduced to tetrahydrofolate in the intestinal mucosa during absorption. • Folate reductase enzyme is required for both these transformation. • Vitamin B6 and C are also required for this reduction
METABOLISM • All forms of Folacin are equally utilized in the body • More Folacin is excreted in urine and feces than is accounted for in the diet , which indicates that this vitamin is also synthesized by intestinal flora • Folacin is mostly stored in liver • Folic acid is converted to its another biologically active form Folinic Acid in the liver
Recommended dietary allowance • RDA for adults is 400 g of folacin daily
Major Function • Folate deficiency leads to “Megaloblastic anemia”.
Important Role in nucleic acid synthesis • Folate is needed to carry one-carbon groups for methylation reactions and nucleic acid synthesis the most notable one being thymine, but also purine bases. • Thus, folate deficiency hinders DNA synthesis and cell division, affecting hematopoietic cells.
RNA transcription, and subsequent protein synthesis, are less affected by folate deficiency, as the mRNA can be recycled and used again as opposed to DNA synthesis, where a new genomic copy must be created.
Macrocytic Anemia • Most characteristic feature of folate deficiency. • During RBC generation, DNA synthesis is delayed. • Protein Synthesis continues. • Hemoglobin accumulates in RBCs precursors. • This dissociation between the maturity of the nucleus and cytoplasm manifest as Immature looking nucleus • While the eosinophilic cytoplasm gets mature in the bone marrow. • RBCs get larger in size, Macrocytosis.
Contd. • Reticulocytosis is often seen. • If the deficiency is severe then even nucleated RBCs are seen the circulation. • These abnormal RBCs are rapidly destroed in the spleen. • This hemolysis leads to low life span of RBCs. • Reduce generation and increased destruction results in anemia • Similar defects in granulocyte lead to hyper-segmentation of neutrophils and leukopenia is the result.
Prevention of Neural Tube Defect leading to spina bifida at the very early stage of pregnancy
Neural Tube Defects Deficiency of folate in pregnant women has been implicated in neural tube defects (NTD); therefore, many developed countries have implemented mandatory folic acid fortification in cereals, etc.
It must be noted that NTDs occur early in pregnancy (first month), therefore women must have abundant folate upon conception. • Folate deficiency as leads to anemia, which further leads to fatigue and weakness and inability to concentrate.
Other Functions • Folic acid is said to be helping in prevention of cancer in females specially Cervical dysplasia. • Folic acid reduce the level of homocystein in blood and therefore useful in preventing heart diseases.
Common symptoms of folate deficiency • Diarrhea • Anemia • Weakness • SoB • Nerve Damage with weakness of limbs • Pregnancy complication • Mental confusion • Depression • Swollen tongue • Mouth ulcers/Peptic ulcer
How Deficiency Develops ? • Folate deficiencies are rare due to the adequate presence of it in the diet. • Poor dietary habits as those of chronic alcoholics can lead to folate deficiency. • Common in pakistani women during pregnancy. • In defective absorption specially in sprue. • Intestinal enzymes deficiency required for the removal of extra glutamyl residues.
Deficiency Diseases • The predominant causes of folate deficiency in non-alcoholics are impaired absorption or metabolism or an increased demand for the vitamin. • Certain drugs such as anticonvulsants and oral contraceptives can impair the absorption of folate. • Anticonvulsants also increase the rate of folate metabolism.
Deficiency Diseases • Folic acid appears to reduce the risk of stroke • Low blood levels of folic acid are associated with increased risk of cancer. (Breast, pancreas and colon) • Damage to DNA caused by folate deficiency may be the reason.
INCREASED REQUIREMENT • The predominant condition requiring an increase in the daily intake of folate is, pregnancy. • pregnancy and infancy are both characterized by increased number of rapidly proliferating cells present in the blood. • The need for folate will nearly double by the third trimester of pregnancy.
Possible Toxic Effect • Risk from Folic acid Toxicity is very low. • Tolerable upper intake level for adult is 1 mg/day. • Upper intake level is 800 ug/day for pregnant and lactating women if less than 18 years of age. • Supplemental level should not increase than the upper level to prevent folic acid from masking symptoms of Vitamin B-12
Toxic Effect • No toxic effect in humans