Download
1 / 73
740 likes | 1.1k Views
Anesthesia For Intracranial Vascular Lesions. By dr : ahmed yehia,md lecture of anesthesiology faculty of medicine- ain shames university. Epidemiology Understand pathophysiology of aneurysms Presentation of I.C aneurysms complications of I.C aneurysms. Objectives.

E N D
By dr: ahmedyehia,mdlecture of anesthesiologyfaculty of medicine-ain shames university
Epidemiology • Understand pathophysiology of aneurysms • Presentation of I.C aneurysms • complications of I.C aneurysms Objectives
Recognize the different treatment modalities of intracranial aneurysms • Understand the basic anesthetic management of intracranial aneurysm clipping • Select an anesthetic plan utilizing medications and or therapies designed to reduce brain injury during cerebral aneurysm repair.
Incidence : 1 to 6% • Incidence of ruptured aneurysm: 12/100,000 • Age: any age, peaks 40 - 60 • Sex: M/F 2:3 • Sites : 30% ICA 40% ACA 20% MCA,10% Vertebro-basilar systems Epidemiology
Causes • Risk Factors • Classification • Locations • Neuronal injury and death Pathophysiology
Causes Intracranial aneurysms are most likely to develop over the course of an individual’s life, with only 10%accountable to a genetic/familialcause, it is primarily acquired90%.
Inherited RF Others • Polycystic kidney disease Over 50 years of age • Type IV EhlerDanlos syndrome Female gender • PseudoxanthomaelasticumSmoking • Neurofibromatosis type 1 Infection of vessel wall • Alpha 1 antitrypsin deficiency Head trauma • Coarctation of the aorta Septic emboli • Fibromuscular dysplasia Hypertension • Pheochromocytoma Alcohol abuse • Klinfelter’s syndrome Oral contraceptive pills • Tuberous sclerosis hypercholesterolemia Risk Factors
True or false • By size: Small: ≤ 10mm Large: 11 to 25mm Giant: > 25mm Classification
By shape: –Saccular –berry aneurysm –Fusiform
Brain Ischemia GlobalFocal Hypoperfusion contains tworegions Vasospasm. 1st region receives no blood flow. 2nd receives collateral flow and is partially ischemic. Neuronal injury and death
Early is excitotoxicity. Ischemia Induced Neuronal Changes
Delayed Is death caused by apoptosis
Ruptured Unruptured (SAH) asymptomatic ICP Hydrocephalus Global,focal neurological deficits Meningeal irritation (initially may be due intracerebral bleeding, or from herniation). Presentation of I.C aneurysms
Rebleeding • Vasospasm • Hydrocephalus • Seizure(seizure prone for 18 months after SAH) Neurological complications
Aneurysmal Rebleeding: Risk : 4% during the first 24 hrs and then 1.5% per day Intraoperative 7% High mortality (78%) IMPAIRED AUTOREGULATION Risk of rebleeding proportional to transmural pressure (MAP-ICP) MAP AVOID
Peaks 5-7 days, resolves after 14 days Angioplasty vasospasm 70%,symptoms 30% Transcranial droppler (TCD) blood velocity changes cerebral ischaemia & infarction Presentation Reversability Severity frequancy Cerebral vasospasm
Management: Triple H therapy +Nimodipine ↑ perfusion pressure & ↓ blood viscosity → CBF ↑ • SBP 120-150 mmhg in unclipped 160-200 mmHg in clipped aneurysm. • CVP 8-12mmHg • HCT 30-35%
Nimodipine V.DOF Collarerals Ca influx 60mg orally every 4 hours, continued for 21days. I.V 1mg/h up to 2mg/h after 6 h SBL.P NOT LESS THAN 150-130 Balloon angioplasty Intraarterial papaverine
Early Late IC H VASOSPASM BLOOD CSF CO2 VS Vasospasm CSF Drainage VS ICP (Rebleed) Hydrocephalus
Clipping Coiling VS Poor HUNT&HESS Co morbidity Basilar Artery
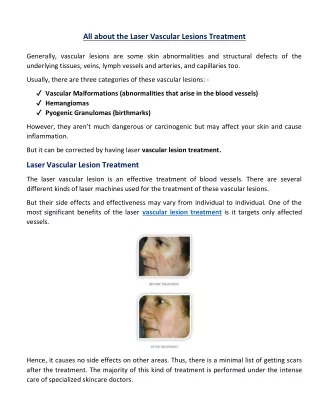
Surgical Treatment- Clipping Aim: isolate the weakened vessel area from the blood supply
Direct Clipping When the surgeon can visualize the surrounding structures, parent vessel and perforators and when the neck is soft
Temporary Clipping SURGICAL PHARMACOLOGY temporary clip is placed on the parent vessel permanent clip is placed on the aneurysm neck temporary clip is removed from the parent vessel
Timing of surgery Late surgery reduces the risk of a further bleed provide excellent operating condition 30% of patients did not survive Early surgery
CVS complications of SAH sympathetic cathecolamine release posterior hypothalamus injury • systemic and pulmonary hypertension, cardiac arrhythmias, • myocardial infarction, and pulmonary oedema. Systemic evaluation
cardiogenic shock. Investigations may reveal an abnormal ECG and elevated cardiac troponin levels. • Management is mainly supportive (inotropes, ventilation), and cardiac dysfunction is reversible in most cases
ECG abnormalities • 25-100% of SAH patients • higher in poor grade patients • T wave inversion & ST depression (most common), • Prolong QT (arterial & ventricular dysrhytmias) • Q waves
Preop echo • serial cardiac enzymes • invasive haemodynamic • monitoring & treatment • Respiratory system • Most common non-neurological cause of death in • SAH • Neurogenic Pulmonary oedema • Atelectasis & pneumonia • Aspiration risk (Loss of consciousness) • Pulmonary embolism (immobility)
Fluid status • More than one third of patients have decrease IV • volume • reduced fluid intake, vomiting • diuretic effect of IV contrast • vasodilatory effect of nimodipine • exacerbates vasospasm & cerebral ischaemia • CVP monitoring in poor grade patients
Electrolytes disturbances Hypopnatraemia 1. Cerebral salt wasting Secretion of brain and atrialnatriuretic peptide IV volume depletion Fluid replacement (normal or hypertonic saline) 2. SIADH Accumulation of excess water with a high CVP Fluid restriction Hypokalaemia,Hypocalcaemia& Hypomagnesaemia
Radiological evaluation • Cerebral Angiogram • Site of the aneurysm • Prepare for intraop positioning, surgical exposure &monitoring • CT scan • Increase ICP from IC haemorrhage, hydrocephalous or cerebral oedema • TCD • facilitate vasospasm management.
Monitoring • Standard monitoring • Intra-arterial line preinduction under LA • Central venous catheter for CVP monitoring • Fluid status & resuscitation, post op Triple H therapy • The use of neurophysiological monitoring, • such as evoked potentials,EEG, has not been shown to improve outcome. • poor predictive value • affected by the use of volatile anaesthetic agents.
SSEPS ANT&POST ANEUYRISM BAEPS POST ANEUYRISM Guide safeTemporary Clipping Detect burst supression
CBF MONITOR Jugular venous bulb monitoring has also not been established and may interfere with cerebral venous drainage. Transcranial droppler (TCD)
Premedication • Continue all usual medications • Pre op sedative medications are best • ICP • omitted(Paco2 &CBF) • Sedate • Poor grade patients : • intubated,ventilated & stable haemodynamic
Avoid increases in transmural aneurysm pressure • Provide good conditions for the aneurysm surgery • a) "slack" brain • b) reduce aneurysmal pressure during clipping • Induced hypotension • Temporary clips • Brain protection The principles
Transmural aneurysm pressure Risk of rupture Risk of ischemia
Prevent changes in transmural pressure (TMP) TPMG= CPP = MAP-ICP MinimiseTPMG to reduce risk of rupture OptimiseCPP to prevent ischemia Maintain BP at pre op levels until the aneurysm is secured ↓ BP by 20-30% tolerable in good grade patients but not in poor grade patients (with ICP ↑& CPP ↓)
Prophylaxis against increased BP during laryngoscopy /intubation IV narcotics, IV lignocaine Antihypertensives (e.glabetolol or esmolol) Ensure full relaxation prior to intubation HOW TO DEAL?
Ensure optimal depth of anesthesia Maintenance of anesthesia IV technique (TIVA/TCI) Low dose volatile agents< 1 MAC + Opoiod Infusion
Highly stimulating interventions: • placement of the pin head holder • raising of the bone flap • dural incision, skin incision & closure • bolus dose of anaesthetics (propofol, thiopentone) • antihypertensives (esmolol, labetolol) • IV narcotics