Download
1 / 10
100 likes | 241 Views
E d. Viral Myocarditis and Dilated Cardiomyopathy. Kristine Scruggs, MD AM Report 10 March 2010. Signs & Symptoms of Myocarditis. Excessive fatigue Chest pain Unexplained sinus tachycardia Acute pericarditis S3, S4 or summation gallop Abnormal electrocardiogram

E N D
E d Viral Myocarditis and Dilated Cardiomyopathy Kristine Scruggs, MD AM Report 10 March 2010
Signs & Symptoms of Myocarditis • Excessive fatigue • Chest pain • Unexplained sinus tachycardia • Acute pericarditis • S3, S4 or summation gallop • Abnormal electrocardiogram • Abnormal echocardiogram • New cardiomegaly on CXR • Atrial or ventricular arrhythmia • Partial or complete heart block • New onset CHF • Atypical MI • Cardiogenic shock • Sudden, unexpected death
Etiologies of DCM (Felker, et al.) • Idiopathic (50%) • Myocarditis (9%) • Viral, Bacterial, Fungal, Protozoal, Helminth • Ischemic heart disease (7%) • Infiltrative disease (5%) • Amyloidosis, Sarcoidosis, Hemochromatosis • Peripartumcardiomyopathy (4%) • Hypertension (4%) • HIV infection (4%) • Connective Tissue Disease(3%) • Scleroderma, SLE, etc • Substance abuse (3%) • Cocaine, EtOH • Doxorubicin (1%) • Other (10%) • Restrictive CM, Familial CM, Valvular heart dz, Endocrine, Neuromuscular, Neoplastic, Drugs (other), Critical illness, etc.
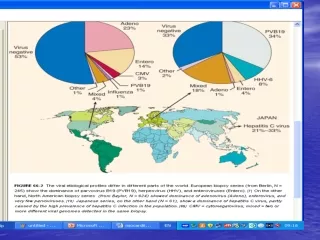
Viral Etiologies of Myocarditis • Enterovirus (e.g. Coxsackie B)* • Adenovirus* • Hepatitis C • CMV • Echovirus • Influenza • EBV • Parvovirus B-19 • HHV-6 *Associated with progression to DCM (Bowles, et al.)
Diagnosis • Serologies • Cultures • PCR (direct examination of cardiac tissue) • Incidence/prevalence of viral myocarditis difficult to assess • No non-invasive “gold standard” • 3.5-5% cardiac involvement during coxsackie outbreak • 6% at autopsy of SCD in young athletes • 149 pts w/ DCM unknown etiology, + PCR in 20% (Bowles, et al) • Versus 1.4% in controls • All adenovirus (60%) and enterovirus (40%) • 1230 pts w/ DCM, mycarditis the cause in 9% (Felker, et al.)
Pathophysiology of Viral Myocarditis --> DCM • Late sequela of acute or chronic viral myocarditis • Due to • direct viral injury (viral toxicity, perforin-mediated cell lysis, cytokine expression) • persistence of virus (initial immune response is protective) • autoimmune phenomenon (“anti-heart” antibodies) • In one study, 93% of patients with myocarditis on biopsy had history of preceding viral illness (Bowles, et al.) • Initial immune response is probably protective • Decreases inflammation • Stronger humoral and cellular immune response linked to less severe initial disease
Take Home Points • Viral infection (esp. with adeno, entero) causes myocarditis in up to 5% of cases • In patients with newly diagnosed DCM, 9% have been traced to viral myocarditis • Incidence/prevalence is difficult to assess as there is no “gold standard” for diagnosis • Damage is caused by direct viral injury, persistent viral infection/inflammation, and auto-immune phenomena. • Prognosis is thought to be generally good, as only the severe cases present with clinical findings • Recent onset IDCM (<6 mo) showed improvement from baseline EF 25% to 42% in one year • Transplant free survival 92% at one year and 88% at two years (McNamara, et al.)
References • Bowles NE, et al. Detection of Viruses in Myocardial Tissues by Polymerase Chain Reaction: Evidence of Adenovirus as a Common Cause of Myocarditis in Children and Adults. J Am Coll of Card. 2003. 42: 3. 466-472. • Cooper LT, et al. Etiology and Pathogenesis of Myocarditis. UpToDate. 2009. • Felker GM, et al. Underlying Causes and Long-term Survival in Patients with Initially Unexplained Cardiomyopathy. New Engl J of Med. 2000. 342: 15. 1077-1081. • McNamara DM, et al. Controlled Trial of Intravenous Immune Globulin in Recent-Onset Dilated Cardiomyopathy. Circulation. 2001; 103:2254-2259.