Download
1 / 42
420 likes | 590 Views
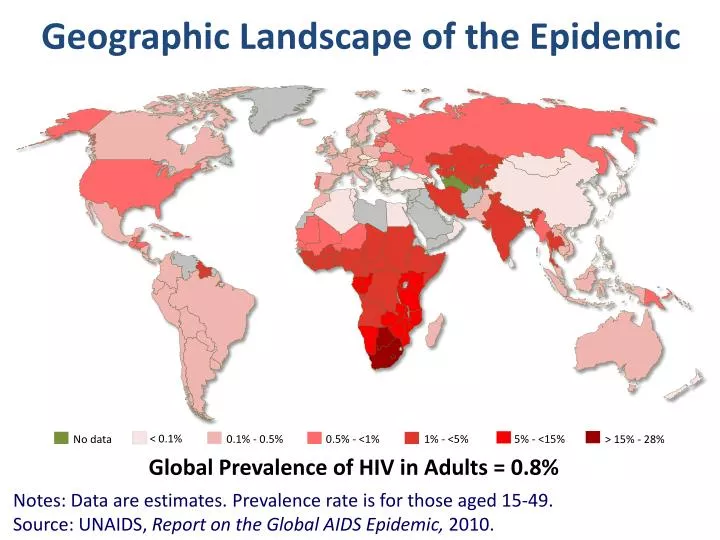
Geographic Landscape of the Epidemic. < 0.1%. 1% - <5%. 0.5% - <1%. 5% - <15%. 0.1% - 0.5%. No data. > 15% - 28%. Global Prevalence of HIV in Adults = 0.8% . Notes: Data are estimates. Prevalence rate is for those aged 15-49. Source: UNAIDS, Report on the Global AIDS Epidemic, 2010.

E N D
Geographic Landscape of the Epidemic < 0.1% 1% - <5% 0.5% - <1% 5% - <15% 0.1% - 0.5% No data > 15% - 28% Global Prevalence of HIV in Adults = 0.8% Notes: Data are estimates. Prevalence rate is for those aged 15-49. Source: UNAIDS, Report on the Global AIDS Epidemic, 2010.
WHO estimates from 2011-2012 • Globally, 34 million people living with HIV in 2012 • Including 3.3 million children less than 15 years • 2.5 millions new infections (including 330 000 children); 22% less than in 2001 • 1.7 million people died of AIDS in 2011 • Each day, 4000 more people on antiretroviral therapy
7,000 New infections every day 1,000 in children
2013 – The HIV Treatment “Math” • Only 8 M HIV(+) people on cART in 2013 • Baseline CD4+ cells often <150/μL in Africa • Clinical consensus: 26 M more need cART now • cART more cost-effective if it also prevents HIV infection by reducing infectiousness • Treatment as prevention sounds terrific, but we struggle with even our inadequate coverage and adherence
Treatment as Prevention: An anchor of combination prevention • Reduced VL correlated with lower sexual transmission • Quinn (2000), Fideli (2001), Vernazza (2000), Donnell (2010), Novitsky (2011), Tanser (2013) • RCT: HPTN 052, discordant couples • Cohen (2011) • PMTCT: Lessons from the first TasP • Reithinger R, et al. Monitoring and evaluation of programmes to prevent mother to child transmission of HIV in Africa. BMJ 2007 • Stringer EM, et al. Monitoring effectiveness of programmes to prevent mother-to-child HIV transmission in lower-income countries. Bull World Health Organ 2008 • Stringer EM, et al; PEARL Study Team. Coverage of nevirapine-based services to prevent mother-to-child HIV transmission in 4 African countries. JAMA 2010
<400 <400 <400 >50 000 >50 000 >50 000 400-3499 400-3499 400-3499 3500-9999 3500-9999 3500-9999 10 000-49 999 10 000-49 999 10 000-49 999 VL and HIV transmission risk in Ugandan discordant couples (linked and unlinked transmissions) 30 M to F Transmission All subjects F to M Transmission 25 20 15 10 Transmission rate per 100 PY 5 0 Viral load (HIV-1 RNA copies/mL) REF: Quinn TC, et al.NEJM 2000
Zambian discordant couples (linked tx only) No transmissions at <3000 VL/mL REF: Fideli US, et al. AIDS Res Hum Retrovir2001
REF: Vernazza PL, et al. AIDS 2000. REVIEW: Cohen & Gay. Clin Infect Dis 2010.
Partners in Prevention HSV/HIV Transmission Study • 3381 HIV-1 discordant heterosexual couples in southern and eastern Africa • Followed 12-24 months, quarterly visits • Intensive couples prevention counseling, free condoms Ref: Celum C, al.N Engl J Med 2010
cART and HIV-1 transmission Adjusted* Relative Risk = 0.08 (95% CI 0.002, 0.57), p = 0.004 * For time on study and CD4 count HIV+ Case: ART-exposed HIV-1 transmission (non-adherence likely) HIV- ART Enrollment 3mo 6mo 9mo 12mo CD4 : 302 201 637 log10VL: 4.7 4.6 4.7 undetermined Donnell D, et al. Lancet 2010;375:2092-8.
Many more persons infected with subtype C have chronic high viremia than reported in other subtypes REF: NovitskyV, Ndung'u T, Wang R, et al. Extended high viremics: …. AIDS 2011; 25:1515-22.
Time series of maps: proportion of the HIV(+) adults & adolescents (≥15 yrs old) on ART (A) and HIV prevalence (B) in surveillance area (using standard Gaussian kernel of radius 3 km) 2005 to 2008, L to R Population-based prospective cohort studies in rural KwaZulu-Natal, South Africa to follow up 16,667 individuals who were HIV-uninfected at baseline, observing HIV seroconversions, 2004 to 2011. 2009 to 2011, L to R Tanser F, et al. Science 2013
Multivariable analysis: HIV(-) individual's HIV aHR (95% CI) for varying ART coverage, i.e., proportion of HIV(+) population receiving ART (A and B), and ambient HIV prevalence (C) (derived w/ standard Gaussian kernel of radius 3 km). Controlling for differences in age/sex distributions Holding key HIV risk factors constant, an HIV(-) individual living in a community with high ART coverage (30-40% of HIV(+)s on ART) was 38% less likely to acquire HIV than where ART coverage was <10%. Also control for community HIV prevalence, marital status, household wealth, # sexual partners past 12 mo Tanser F, et al. Science 2013
HPTN 052 Study Design HIV-infected subjects with CD4 350 to 550 cells/mm3 1763 serodiscordant couples Randomization Immediate ART CD4 350-550 Delayed ART CD4 <250 N = 886 N = 877 All 886 initiated therapy at the start 184 initiated therapy during the trial REF: Cohen MS, et al. N Engl J Med 2011.
HPTN 052 results Total HIV-1 Transmission Events: 39 Linked Transmissions: 28 Unlinked or TBD Transmissions: 11 • 64% transmissions (tx) from HIV+ w/ CD4 >350 cells/µL & VL >50,000 c/mL • 82% (23) tx from sub-Saharan Africa • 64% (18) tx from ♀ to ♂ partners Immediate Arm: 1* Delayed Arm: 27 p < 0.001 Cohen MS, et al. N Engl J Med 2011. * Tx likely near time of cART initiation
HIV Suppression Stops Transmission “HPTN 052 is a game changer” Michel SidibeExecutive Director of UNAIDS Note: adherence to cART was very high in this well-funded RCT “How do we pull this off in the real world?” Jim Shelton Science 2011 96% reduction in the risk of transmission to sexual partners
IOM Committee on Perinatal Transmission of HIV ACTG 076 Wortley PM, et al. Successful implementation of perinatal HIV prevention…. MMWR 2001 Lansky A, et al. Trends in HIV testing among pregnant women….Am J Public Health. 2001 Lindegren ML, et al. Trends in perinatal transmission of HIV/AIDS in the US. JAMA. 1999
New HIV infections among children, 1990-2007 (2008 UNAIDS) HIVNET 012 • Still, >1000 babies infected with HIV every day: 370,000 in 2009, 98% in LMICs UNAIDS 2010
↑ Nevirapine coverage in Zambia Pregnant, HIV+ Women Women must access ANC ANC must have VCT/NVP available (90%) Offered Intervention Mother must agree to the intervention (80%) Uptake Intervention Mother must take the pill at labor (60%) Adhere to Intervention Mother & baby have both been given NVP Nurses must give the baby NVP (70%) 30%! Refs:JAIDS2000.24: 369; AJPH 2002.92:365;Lancet 2001.358:1611;AIDS2003.17:1377;AIDS2003.17165:9; Lancet 2003.362:667&1850; JAIDS2004.35:60; AIDS2004.18:939; AIDS2005.19: 1309; BMJ2007.334:1143; AIDS2007.21:957; BMJ2007.334:1143; AJOG 2007.197:e1. AIDS 2007.21:957; NEJM 2008.359:130;JAIDS 2008.47:79. JAIDS 2009.52:273; AIDS 2010.24:447; AJE 2010.171:924.
Do we really know how to increase coverage and adherence? This is a new HIV prevention research paradigm! ↑ Nevirapine coverage in Zambia Pregnant, HIV+ Women Women must access ANC ANC must have VCT/NVP available (90%) Offered Intervention Mother must agree to the intervention (80%) Uptake Intervention Mother must take the pill at labor (60%) Adhere to Intervention Mother & baby have both been given NVP Nurses must give the baby NVP (70%) 30%! Refs:JAIDS2000.24: 369; AJPH 2002.92:365;Lancet 2001.358:1611;AIDS2003.17:1377;AIDS2003.17165:9; Lancet 2003.362:667&1850; JAIDS2004.35:60; AIDS2004.18:939; AIDS2005.19: 1309; BMJ2007.334:1143; AIDS2007.21:957; BMJ2007.334:1143; AJOG 2007.197:e1. AIDS 2007.21:957; NEJM 2008.359:130;JAIDS 2008.47:79. JAIDS 2009.52:273; AIDS 2010.24:447; AJE 2010.171:924.
QI to expand PEPFAR coverage • Infant retention poor, limiting early infant diagnosis (EID) in rural Zambézia Province, Mozambique • Only 25% all HIV-exposed infants made initial visit for testing • 49% all HIV-infected mothers retained in HIV-related care REF: Cook RE, et al. JAIDS 2011
Process Map: PMTCT Woman Presents Maternity Ward Woman/ Infant Return 1 month EID Clinic HIV Status Ascertained Routine Care N HIV Pos? Infant Enrolled/ Record Initiated Y Infant Examined Prophylaxis Given PCR Test Drawn Infant Delivered Counseling Given Prophylaxis Given Discharge Discharge Counseling/EID Referral |----- <50 m -----| Ciampa PJ, et al. JAIDS 2011 and 2012
Process Map: PMTCT Services (Enhanced Referral) Woman Presents vv Woman/ Infant Return 1 month EID Clinic Maternity Ward HIV Status Ascertained Routine Care N HIV Pos? Infant Examined N Prophylaxis Given Counseling/EID Referral Counseling Given Y Infant Delivered Direct Accompaniment Infant Enrolled/ Record Initiated PCR Drawn Prophylaxis Given Discharge Discharge |-- <50 m --| Ciampa PJ, et al. JAIDS 2011 and 2012
Results from expanded QI • N= 791 women/infants • (168 in phase 2) • REFS: Ciampa PJ, et al. JAIDS 2011 and JAIDS 2012. Kaplan-Meier estimates of time from birth to access of EID forHIV-exposed infants pre-post intervention phases (A), and by receipt ofenhanced vs. standard referral (B)
Testing and linkage to care Initiation of ART Testing Adherence to ART Positive Prevention Linkage to care sites Decrease in HIV Transmission Test HIV + Adopt safer behaviors Enroll in Care Treat Maintain viral suppression
100 HIV+ persons Objective Achieved Not Achieved Aware HIV+79% Not Virally Suppressed 79 21 Linked to care60% 47 32 53 Viral Load suppressed 55% 26 21 74 NOTE: Only 26% of HIV+ persons in 2009 were in care with an estimated VL <500 copies/mL. REF: Burns DN, Dieffenbach C, Vermund SH. Clin Infect Dis 2010; 51:725-31.
Treat to prevent: Aspiration Meets Reality 80% 77% 66% 89% 77% Multiplies to 28% Only 28% of HIV+ Americans had optimal suppression in 2010Refs: Gardner, ClinInf Dis2011 MMWR 2011
Aspiration Meets Reality 80% INCREASE RETENTION 77% 66% 89% 77% EARLY cART BETTER LINKAGE Multiplies to 28% INCREASE ADHERENCE MORE TESTING
Testing and linkage to care Co-morbidities lead to: Increased transmission Less testing Less linkage Less retention Less treatment Less adherence Less VL suppression Initiation of ART Testing Adherence to ART Positive Prevention Linkage to care sites Decrease in HIV Transmission Test HIV + Adopt safer behaviors Enroll in Care Treat Maintain viral suppression
High income settings: Maximizing the HIV Prevention, Care and Treatment Continuum Primary Prevention Efforts HIV • PrEP, PEP, condoms, syringes • Drivers • Substance use • Alcohol • Meth • Crack • Poppers • STDs, # of partners Engagement / Retention Engagement / Retention Linkage Treatment Adherence Mental Health Services Routine Medical Testing Medical Case Management Substance Use Treatment Linkage & Partner Services ART Guidelines Uptake Community Testing Housing Support STD & PCSI SFDPH Positive Health Access to Services and Treatment (PHAST) Engagement & Partner Services REF: Das M, et al. PLoS One 2010
HPTN 071 - PopART Study Population effect of universal testing and immediate ART therapy to Reduce HIV Transmission
Hypothesis Universal voluntary HIV testing with appropriate combination prevention offered to all those testing HIV negative - in addition to immediate ART for all those testing HIV positive - will have a substantial impact on HIV incidence at population level
The PopART Combination Intervention Package • Universal voluntary annual home-based HIV testing • Linkage to care (local health center) for those testing HIV(+) • Immediate ART offered to those testing HIV positive • Voluntary medical male circumcision for men testing HIV(-) • Strengthening and promoting PMTCT services • Syndromic STI treatment at clinic • Drug and alcohol use assessment • Counseling and condom provision in the community Community HIV Providers (CHiPs) to deliver testing, counselling, linkage to care, & treatment support in the community
Trial Design: three-arm, two-country, cluster-randomized • 21 clusters (communities): 12 in Zambia, 9 in So. Africa • Average of ~50,000 in each cluster; 50% are adults • Incidence measured in Population Cohort: 2,500 adults in each cluster, followed up yearly for 3 years
HPTN 071/PopART Study Design:A 3-Arm, 2-Country Cluster Randomized Trial 15-30,000 adults in each community B C A B C A A B C A Enroll 2.500 into Population Cohort B Zambia C A A South Africa B B C C C A B
Study Locations: • 12 communities in Zambia • 9 communities in the Western Cape of South Africa Zambia South Africa
Objectives • Primary Objective • To measure the impact of the PopART intervention in reducing HIV incidence • Measured in a cohort of 52,500 adults over 3 years • Secondary Objectives • Uptake of intervention components • Retention in HIV care • Sexual risk behavior • HIV-related stigma • HIV disease progression and death • TB case notification rate • HSV-2 incidence • ART Toxicity • ART adherence and viral suppression * • Community viral load* • ART drug resistance* *if further funding obtained
The HPTN 071 Study Team, led by: Dr. Richard Hayes, Protocol Chair, LSHTM Dr. Sarah Fidler. Protocol Co-Chair, Imperial College Dr. Helen Ayles, Zambia PI, Zambart Dr. NuldaBeyers, South Africa PI, Desmond Tutu TB Center
Sister study to HPTN 071/PopART here at the Harvard School of Public Health • The Botswana Combination Prevention Project (BCPP) • Max Essex, Victor DeGruttola, Joseph Makhema, many colleagues and partners, Botswana MoH • Key conceptual difference: Use VL to choose persons to treat to achieve increased efficiency and focus for the intervention • Careful harmonization efforts with PopART • Smaller studies addressing similar issues: see GranichR et al; ART in Prevention of HIV &TB Research Writing Group. ART in prevention of HIV/TB: update on current research…. Curr HIV Res 2011
HPTN 065: TLC-Plus in the US Social Mobilization
Why is a Trial Needed? • Not known whether a UTT intervention can be delivered with high uptake and acceptability • Many uncertainties in model parameters • Population-level impact of intervention package is not known • Potential adverse effects such as sexual risk disinhibition, HIV-related stigma, overload of health services, toxicity, and drug resistance • A rigorously designed trial can measure the costs and benefits of this strategy and provide reliable evidence on cost-effectiveness for health policy makers
2012 Timeline (July 2013 start anticipated) Preparatory phase 2017 2016 2015 2014 2013 CHiPs Intervention Initial Household Visits Return Household Visits Intervention activities Return Household Visits Return Household Visits Population Cohort Enrollment and Survey Return Visit and Survey Return Visit and Survey Return Visit and Survey Analysis & reporting Analysis & reporting Milestone review during 2014 to determine trial continuation in 2016
