Download
1 / 16
160 likes | 192 Views
Explore the redefinition of airflow obstruction in COPD, characterized by reversibility and hyperinflation, impacting diagnosis and treatment of this progressive disease. Discover key findings and guidelines.

E N D
Reversibility: Redefining Airflow Obstruction in COPD ©AstraZeneca LP. All rights reserved. 286850 8/09
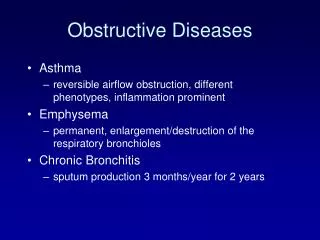
Current Definition and Diagnosis of COPD • A preventable and treatable disease • Associated with significant extrapulmonary effects and important comorbid conditions • Characterized by airflow limitation that is • Partially reversible • Usually progressive • Associated with an abnormal inflammatory response to noxious particles or gases • Postbronchodilator FEV1/FVC <0.7 used to help establish diagnosis Global Initiative for Chronic Obstructive Lung Disease. http://www.goldcopd.com/Guidelineitem.asp?l1=2&l2=1&intId=989. Accessed November 21, 2008.
How is Reversibility of Airflow Obstruction Defined? • Defined by ATS/ERS Task Force on Lung Function Testing1 • Postbronchodilator FEV1 and/or FVC ≥200 mL and 12% improvement over baseline is considered significant bronchodilation1 • GOLD COPD Guidelines have adopted this standard2 1. Pellegrino R, Viegi G, Brusasco V et a. Eur Respir J. 2005;26:948–968.2. Global Initiative for Chronic Obstructive Lung Disease. http://www.goldcopd.org/guidelineitem.asp?l1=2&l2=1&intld=2003. Accessed November 21, 2008.
Hyperinflation Is a Hallmark of COPD Increases FRC (EELV) Decreases IC Increases volume at which tidal breathing occurs Worsens with exercise and reduces exercise tolerance (dynamic hyperinflation) Total Lung Capacity IC Tidal Ventilation FRC (EELV) No Bronchodilator With Bronchodilator HealthyPatients PatientsWith COPD Patients With COPD During Exercise IC = inspiratory capacity; FRC/EELV = functional residual capacity/end expiratory lung volume. Adapted with permission from Sutherland ER et al. N Engl J Med. 2004;350:2689-2697.
Airflow Obstruction Is a Central Feature of COPD1,2 Airflow Limitation, Air Trapping, Lung Hyperinflation, Mucus Hypersecretion Dyspnea Exercise Tolerance Exacerbations Inactivity Decline in Lung Function Deterioration in Health Status Premature Mortality 1. Global Initiative for Chronic Obstructive Lung Disease. http://www.goldcopd.org/guidelineitem.asp?l1=2&l2=1&intld=2003. Accessed November 21, 2008.2. American Thoracic Society, European Respiratory Society. http://www.thoracic.org/sections/copd/. Accessed November 19, 2008.
Asthma and COPD Have Varying Degrees of Bronchodilator Responsiveness 0.8 0.7 ■ 0.6 ■ ■ 0.5 Δ FEV1 0.4 ■ 0.3 ▲ ▲ ▲ 0.2 ▲ 0.1 0 10 100 1000 Cumulative Dose (µg) ■ ▲ Patients With Asthma Ipratropium (anticholinergic) Patients With Asthma Albuterol (β2-Agonist) Patients With COPD Ipratropium (anticholinergic) Patients With COPD Albuterol (β2-Agonist) n=19. Adapted with permission from Higgins BG et al.Eur Resp J. 1991;4:415-420.
COPD Previously Defined as “Irreversible” Airway Obstruction Chronic Bronchitis Emphysema COPD (Irreversible) (Reversible) Airflow Obstruction Asthma Note: Actual subset sizes were not proportional relative to the subset images. Adapted from American Thoracic Society. Am J Respir Crit Care Med. 1995;152(5 pt 2):S77-S121.
Patient Populations Included in COPDStudies Were Largely “Irreversible” Lung Health Study Subject Demographics and Baseline Characteristics n=5887. SIA=smoking intervention and inhaled bronchodilator ipratropium bromide.SIP = smoking intervention plus placebo.UC=usual care. Anthonisen NR et al. JAMA. 1994;272:1497-1505. Mean Reversibility ~4%
“Irreversible” Patients Can ChangeTheir Reversibility Status Over Time Study Population: 660 Patients Meeting Both ERS and ATS Criteria for Irreversible COPD, 40-75 Years of Age, Current or Ex-tobacco Smokers = Positive responders Total % Not Reversible at Each Visit = Negative responders N = 660 Visit 0: 58% Visit 1: 62% Visit 2: 59% 385 275 287 98 121 154 213 74 48 50 75 46 51 103 52% of Patients Changed Bronchodilator Responder Status Over a 2-month Period per ATS Criteria Calverley PM et al. Thorax. 2003;58:659-664.
Albuterol only Ipratropium only Both Neither Reversibility Varies by Patientand Bronchodilator 73% of Patients Show Reversibility to Short-acting Bronchodilators* 11% (n=91) 35% (n=280) 27% (n=222) 27% (n=217) N=813.*Reversibility defined as ≥12% and >200 mL increase in FEV1. Donohue J et al. Presented at the 1997 International Conference of the American Thoracic Society. San Francisco, CA; May 18-21, 1997.
-30 -25 -20 -15 -10 -5 0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 100 A Recent Study Also Demonstrates Reversibility in Many Patients With COPD 15 Degree of Reversibility * *65.6% showed a >15% increase in FEV1 10 Patients, % 5 0 Change in FEV1 % ~54% of Patients Met ATS Reversibility Criteria (≥12% + ≥200 mL) Postbronchodilator FEV1 measured after administration of 80 µg ipratropium and 400 µg albuterol. Adapted with permission from Tashkin DP et al. Eur Resp J. 2008;31:742-750.
Bronchodilators Play an Important Rolein COPD Treatment AlgorithmsATS/ERS Guidelines Confirm Dx of COPD Intermittent Sx (cough, wheeze, dyspnea) SA-BD p.r.n. Persistent Sx (dyspnea, pm awakenings) LA-BD/SA-BD q.i.d. with rescue Limited Benefit? Yes Alternative class/combination (LA-BD/ICS) Limited Benefit? AE? Yes Add/substitute oral theophylline SA-BD = short-acting bronchodilator; LA-BD = long-acting bronchodilator;ICS = inhaled corticosteroid. Adapted from Celli B et al. Eur Respir J. 2004;23:932-946.
Bronchodilatory Response Varies in COPDLong-acting β2-agonist vs Long-acting Anticholinergic 1.8 Form 12 µg bid Tio 18 µg qd 1.7 1.6 FEV1 (mL) 1.5 1.4 AUC FEV1 0-2 hours; Formoterol +114 mL vs tiotropium (P=0.014) 1.3 0 60 120 180 240 300 360 420 480 540 600 660 720 Time (min) n=81. Form = formoterol.Tio = tiotropium. Richter K et al. Respiration. 2006;73:414-419.
Predose Postdose Significant Improvements in Volume-based Measurements After Bronchodilator 800 600 * * 400 * * * * 200 0 Difference (T – P) at Day 28 (mL) -200 -400 * -600 * -800 FEV1 FVC IC FRC Flow Volume n=80. T = tiotropium; P = placebo; FRC = functional residual capacity.*P<0.01. Celli B et al. Chest. 2003;124:1743-1748.
Responders Poor Responders Patients May Respond to Long-term Bronchodilator Therapy, Regardless of Initial Reversibility Status Day 1 Day 344 1.4 1.5 Placebo Tiotropium Placebo Tiotropium 1.4 1.3 1.3 * 1.2 FEV1 (liters) FEV1 (liters) 1.2 1.1 * 1.1 1.0 1.0 -60 -5 30 60 120 180 -60 -5 30 60 120 180 Time (minutes) Time (minutes) n=921. *P<.001 vs placebo at all time points following drug administration. Tashkin D, Kesten S. Chest. 2003;123:1441-1449.
Understanding Reversibility in COPD • Professional guidelines and clinical data demonstrate that airflow obstruction in COPD is at least partially reversible • Studies show that bronchodilators can improve lung function in COPD patients • Reversibility status may vary in response to different bronchodilators, and may change over time • Patients may respond to long-term bronchodilator therapy, regardless of short-term reversibility