Download
1 / 35
490 likes | 1.69k Views
BRUCELLOSIS. Hail M. Al-Abdely, M.D. Associate Consultant Infectious Diseases. Historical Background. Malta Fever Major health problem to British troops in Malta in the 19 th and early 20 th centuries. Historical Background.

E N D
BRUCELLOSIS Hail M. Al-Abdely, M.D. Associate Consultant Infectious Diseases
Historical Background • Malta Fever • Major health problem to British troops in Malta in the 19th and early 20th centuries.
Historical Background • 1860 J.A. Maraston; assistant surgeon in the British Army in Malta -- first accurate description “Mediterranian Gastric Remittent Fever” • David Bruce (1855-1931) -1883 sent to Malta to provide medical care to the troops. - 1887 isolated “micrococcus” from spleens of 4 soldiers died of the disease.
Historical Background • 1897 A.E. Wright ; pathologist in British army - developed agglutination test. What is the source? “Mediterranean Fever Commission” 1904
Historical Background • 1905 Zammit;Maltese physician - Goats were the source of infection. • 1897 E. Bang;Danish veterinarian -described intracelular pathogen causing abortion in cattle named “Bacillus abortus”. • 1918 A. Evans;American microbiologist -made the connection between Bacillus abortus and micrococcus melitensis & named it Bacteriaceae.
Historical Background • 1920 Meyer and Shaw suggested BRUCELLA • 1914 Mohler isolated organism from liver & spleen of Pigs--B.suis. • 1957 B. neotome, 1963 B. ovis, 1966 B. canis
Epidemiology • Worldwide zoonosis • Only 17 countries declared brucellosis free1986 • Six species 1. B.abortus - mainly cattle 2. B.melitensis - sheeps & goats 3. B.suis - pigs 4. B. canis - dogs 5. B. ovis - sheep (not human pathogen) 6. B. neotomae - desert wood rat (not human pathogen) • B. melitensis -- most common worldwide
Epidemiology in Saudi Arabia • Endemic disease • Mostly B. melitensis & b. abortus. • No clear figures about incidence & prevalence. • Incidence : 5.4 per 1000 per year. • Prevalence : 8.6 - 38 % - some regions.
Bacteriology • Gm - ve cocci, coccobacilli, bacilli. • Strict aerobic, nonmotile, nonspore forming. • B. ovis, B. abortus --CO2 supplementation. • Grow in regular media -- prolonged incubation > 4 weeks.
Bacteriology • Surface lipopolysccharide cell wall • smooth vs non-smooth. • determine virulence. • smooth LPS : B. melitensis,suis,abortus • Non-smooth LPS B.canis, ovis. • the basis for agglutination test.
Transmission • Zoonosis affecting domestic animals. • Concentrated in milk, urine, genital organs. ROUTES OF TRANSMISSION • Oral: unpasteurised milk & products raw milk or meet. • Respiratory: lab workers. • Skin: accidental penetration or abrasion • - at risk farmers & veterinarians. • Other routes: Conjunctival, Blood transfusion, Transplacental, ? person to person.
Pathogenesis Entry to the body Macrophage activation Polymorph migration & Phagocytosis Intracelluar multiplication Lymphatics RES organs Blood Any organ
Pathogenesis • Cell mediated immunity also activated with granuloma formation (mainly with B. abortus) • Humoral antibody response of little importance • Main way of body control of the infection is through committed T-lymphocytes producing lymphokines (- Interferon) which activate macrophage killing • Pyogenic infection more with B. melitensis and B. suis
Clinical Manifestations • Incubation period: variable 2- 8 wks. • Presentation: acute 50% & insidious 50% • Sx & signs not specific. • Can affect any organ. • Common nonspecific Sx: - fever with rigors. - sweats, malaise, anorexia. - headache, back pain.
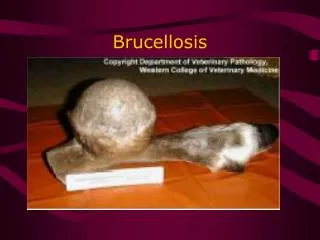
Clinical Manifestations • GIT 70% : anorexia, abd. pain, vomiting, diarrhea,contipation, hepatosplenomegaly. • LIVER : Involved in most cases but LFTs normal or mildly abnormal. • granulomas (B. abortus). • hepatitis (B.melitensis). • abscesses (B.suis).
Clinical Manifestations • Skeletal 20-60% : • arthritis, spondylitis, osteomyelitis. • sacroiliitis - most common. • athritis - oligoarticular : hip, knee & ankles. Joint asp. - monocytosis, culture +ve in 50 %
Clinical Manifestations • Neurologic • Meningitis, encephalitis, radiculopathy & peripheral neuropathy, intracerebral abscesses • Meningitis • acute or chronic • neck rigidity < 50% • CSF • lymphocytic pleocytosis • (N) or low sugar • increase protein • culture +ve < 50% • agglutination +ve in >95%
Clinical Manifestations • Cardiovascular • Edocarditis 2% (major cause of mortality) • Rx: valve replacement and antibiotics • Pericarditis & myocarditis • Pulmonary • Inhalation or hematogenous • Cause any chest syndrome • Rarely Brucella isolated from sputum
Clinical Manifestations • Genitourinary • Epidydemoorchitis • Pyonephrosis (rare) • Cutaneous • Nonspecific • Hematologic • Anemia • Leukopenia • Thrombocytopenia
Diagnosis • History of animal contact is pivotal • In endemic area, it should be in the DDx of any nonspecific febrile illness
Diagnosis • Laboratory • WBC (N) or . monocytosis • ESR of little help • Blood cultures • slow growth = 4 weeks • new automated system BATEC identifies he organism 4-8 days • more recent (BACT/ALERT) - 2.8 days • PCR
Diagnosis • Serology • Main laboratory method of diagnosis • Serum agglutination test - most widely used • measures agglutination for IgG, IgM, IgA • 2ME - break sulf-hydrile bonds in IgM polymer - no agglutination • which level is diagnostic ?? 1 : 160 - non endemic area 1 : 320 - endemic area • SAT - false negative • Prozone • Blocking antibodies • Other tests: coombs, ELISA, CFT, FTA
S IgM
Brucella Antibodies • AGG = IgG + IgM • 2ME = IgG
Prognosis • Preantibiotic era • Mortality 2% mainly endocarditis • Morbidity • High with B. melitensis • Nerve deafness • Spinal cord damage
Prevention • Control of disease in domestic animals • immunization using B. abortus strain 19 and B. melitensis strain Rev 1 • Routine pasteurization of milk • In labs strict biosafety precautions
Treatment Drugs against Brucella • Tetracyclines • Aminoglycosides • Streptomycin since 1947 • Gentamicin • Netilmicin • Rifampicin • Quinolones - ciprofloxacin • ?3rd generation cephalosporins
Treatment Drugs against Brucella • Treatment for uncomplicated Brucellosis • Stremptomycin + Doxycycline for 6 weeks • ? TMP/SMX + Doxycycline for 6 weeks • WHO recommendation 1986 • Rifampicin + Doxycycline for 6 weeks • Treatment of complicated Brucellosis • Endocarditis, meningitis • No uniform agreement • Usually 3 antibrucella drugs for 3 months
Treated Brucellosis Treatment
Relapse Predictors of Relapse Male sex Inadequate antibiotic therapy. Positive culture on initial disease Thrombocytopenia Ariza, et al: CID 20:1241, 1995