Download
1 / 23
310 likes | 690 Views
Martini’s Visual Anatomy and Physiology First Edition Martini w Ober. Chapter 18 The Heart and Cardiovascular Function Lecture 3. Lecture Overview. Physiology of cardiac muscle contraction The electrocardiogram Cardiac Output Regulation of the cardiac cycle and cardiac output.

E N D
Martini’s Visual Anatomy and Physiology First Edition Martini w Ober Chapter 18The Heart and Cardiovascular Function Lecture 3
Lecture Overview • Physiology of cardiac muscle contraction • The electrocardiogram • Cardiac Output • Regulation of the cardiac cycle and cardiac output
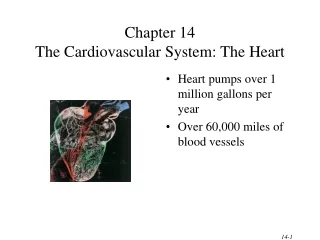
Comparison of Skeletal and Cardiac Muscle • Cardiac and skeletal muscle differ in: • Nature of action potential • Source of Ca2+ • Duration of contraction Figure from: Martini, Anatomy & Physiology, Prentice Hall, 2001 Let’s look at this more closely
The Cardiac Muscle Action Potential • Ca2+ ions enter from • Extracellular fluid (20%) • Sarcoplasmic reticulum (80%) • ** Cardiac muscle is very sensitive to Ca2+ changes in extracellular fluid Recall that tetanic contractions usually cannot occur in a normal cardiac muscle cell Figure from: Martini, Anatomy & Physiology, Prentice Hall, 2001
Electrocardiogram • recording of electrical changes that occur in the myocardium during the cardiac cycle • used to assess heart’s ability to conduct impulses, heart enlargement, and myocardial damage Important points to remember: - Depolarization precedes contraction - Repolarization precedes relaxation P wave – atrial depolarization QRS wave – ventricular depolarization T wave – ventricular repolarization Three waves per heartbeat
Electrocardiogram PR Interval: 0.12 – 0.20 sec QT Interval: 0.20 – 0.40 sec QRS Interval: < 0.10 sec Figure from: Martini, Anatomy & Physiology, Prentice Hall, 2001
Review of Events of the Cardiac Cycle Figure from: Martini, Anatomy & Physiology, Prentice Hall, 2004 • Atrial contraction begins • Atria eject blood into ventricles • Atrial systole ends; AV valves close (S1) • Isovolumetric ventricular contraction • Ventricular ejection occurs • Semilunar valves close (S2) • Isovolumetric relaxation occurs • AV valves open; passive atrial filling S2 S1
Cardiodynamics – Important terms • End-diastolic volume (EDV) – amount of blood present in the ventricles at end of ventricular diastole (~ 120 ml) • End-systolic volume (ESV) – amount of blood left in ventricles at end of ventricular systole (~ 50 ml) • Stroke volume (SV) – amount of blood pumped out of each ventricle during a single beat (SV =EDV – ESV) (~ 70 ml) • Ejection fraction – Percentage of EDV represented by the SV (SV/EDV) (~ 55%)
Cardiac Output (CO) • The volume of blood pumped by each ventricle in one minute CO = heart rate (HR) x stroke volume (SV) ml/min beats/min ml/beat Example: CO = 72 bpm x 75ml/beat 5,500 ml/min Normal CO 5-6 liters (5,000-6,000 ml) per minute
Regulation of Cardiac Output CO = heart rate (HR) x stroke volume (SV) Figure from: Martini, Anatomy & Physiology, Prentice Hall, 2001 SV =EDV – ESV • physical exercise • body temperature • concentration of various ions • calcium • potassium • parasympathetic impulses (vagus nerves) decrease heart action • sympathetic impulses increase heart action; epinephrine
Regulation of Cardiac Rate Autonomic nerve impulses alter the activities of the S-A and A-V nodes Rising blood pressure stimulates baroreceptors to reduce cardiac output via parasympathetic stimulation Stretching of vena cava near right atrium leads to increased cardiac output via sympathetic stimulation Figure from: Hole’s Human A&P, 12th edition, 2010
Regulation of Cardiac Rate Tachycardia > 100 bpmBradycardia < 60 bpm Parasympathetic impulses reduce CO, sympathetic impulses increase CO **ANS activity does not ‘make’ the heart beat, it only regulates its beat Figure from: Martini, Anatomy & Physiology, Prentice Hall, 2004
Additional Terms to Know… • Preload • Degree of tension on heart muscle before it contracts (i.e., length of sarcomeres) • The end diastolic pressure (EDP) • Afterload • Load against which the cardiac muscle exerts its contractile force • Pressure in the artery leading from the ventricle
The Frank-Starling Mechanism • Amount of blood pumped by the heart each minute (CO) is almost entirely determined by the venous return • Frank-Starling mechanism • Intrinsic ability of the heart to adapt to increasing volumes of inflowing blood • Cardiac muscle reacts to increased stretching (venous filling) by contracting more forcefully • Increased stretch of cardiac muscle causes optimum overlap of cardiac muscle (length-tension relationship)
Factors Affecting Cardiac Output Figure adapted from: Aaronson & Ward, The Cardiovascular System at a Glance, Blackwell Publishing, 2007 ANSParasympathetic Sympathetic HR Contractility CO = HR x SV ESV Afterload = EDV - ESV SV EDV CVP CO – Cardiac Output (~5L/min). Dependent upon Stroke Volume (SV; ~70 ml) and Heart Rate (HR) CVP – Central Venous Pressure; Pressure in vena cava near the right atrium (affects preload; Starling mechanism) Contractility – Increase in force of muscle contraction without a change in starting length of sarcomeres Afterload – Load against which the heart must pump, i.e., pressure in pulmonary artery or aorta ESV – End Systolic Volume; Volume of blood left in heart after it has ejected blood (~50 ml) EDV – End Diastolic Volume; Volume of blood in the ventricle before contraction (~120-140 ml)
Regulation of Cardiac Output Recall: SV = EDV - ESV Figure from: Martini, Anatomy & Physiology, Prentice Hall, 2001 CO = heart rate (HR) x stroke volume (SV) Be sure to review, and be able to use, this summary chart
Life-Span Changes • deposition of cholesterol in blood vessels • cardiac muscle cells die • heart enlarges • fibrous connective tissue of heart increases • adipose tissue of heart increases • blood pressure increases • resting heart rate decreases
Review • Cardiac muscle contraction differs in several important ways from skeletal muscle contraction • Duration of the action potential is longer • Ca2+ for contraction is derived from the extracellular fluid as well as the sacroplasmic reticulum • Length of contraction is longer • Tetany cannot develop due to length of the absolute refractory period • The electrocardiogram • Measures the electrical changes occurring in the heart • Is used to assess heart’s ability to conduct impulses, heart enlargement, and myocardial damage • Depolarization -> contraction, repolarization -> relaxation
Review • There are three major events (waves) in the ECG • P wave = atrial depolarization • QRS complex = ventricular depolarization • T wave = ventricular repolarization • The different leads of an ECG can be used to localize heart muscle abnormalities • Abnormalities in ECG presentation can be indicative of heart damage • Several common cardiac abnormalities • Arrhythmia • Tachycardia (and bradycardia) • Atrial flutter
Review • Important cardiodynamic terminology • End-diastolic volume (EDV) – amount of blood left in ventricles at end of ventricular diastole • End-systolic volume (ESV) – amount of blood left in ventricles at end of ventricular systole • Stroke volume (SV) – amount of blood pumped out of each ventricle during a single beat (EDV – ESV = SV) • Ejection fraction – Percentage of EDV represented by the SV
Review • Cardiac output (CO) • Amount of blood pumped by the heart in one minute • CO = stroke volume x heart rate • Normal (resting) CO 5-6 L/min • Factors Affecting CO • Autonomic activity • Hormones • K+, Ca2+ • Venous return
Review • Regulation of Cardiac Output • Heart Rate • Autonomic tone • Hormones • Venous return • Stroke Volume • Autonomic tone • Hormones • Venous return • Afterload